
When you get a paper cut or scrape your knee, you expect it to heal.Your body has a remarkable, built-in repair system that kicks into gear, patching things up in a predictable order. But what happens when that system breaks down and a wound just… stays?
That’s the reality of a chronic wound. It’s not just a slow-healing injury; it’s one that has become stuck, failing to move through the normal healing process within the expected four to six weeks. This stall is a major red flag, signaling a deeper, underlying problem that’s preventing your body from doing its job.
Understanding Why Some Wounds Never Heal
Think of a simple cut—what clinicians call an acute wound—like a well-organized construction project. The moment the injury happens, specialized crews (your cells) arrive on schedule. They clear out the debris, lay a new foundation of tissue, and methodically rebuild the structure until the job is done.
A chronic wound is like that same construction project, but with a persistent roadblock. The crews show up, but they can’t get past the first stage. They remain stuck in a state of inflammation, unable to start rebuilding. The site stays open, vulnerable, and in a constant state of distress.
Acute vs Chronic Wounds at a Glance
This fundamental difference is why a chronic wound demands specialized medical attention. While your body can handle a minor scrape on its own, a non-healing wound is a sign that it needs expert help to clear the roadblock and restart the healing engine.
Let’s break down the key differences.
| Characteristic | Acute Wound (e.g., paper cut, minor scrape) | Chronic Wound (e.g., diabetic ulcer, pressure sore) |
|---|---|---|
| Healing Time | Follows a predictable timeline, healing within 4-6 weeks. | Becomes stalled and lasts longer than 6 weeks. |
| Underlying Cause | Usually from simple, external trauma. | Linked to underlying health conditions like diabetes or poor circulation. |
| Healing Process | Moves smoothly through the four stages of healing. | Gets stuck, typically in the inflammatory phase. |
| Outcome | Heals completely, often with minimal scarring. | Fails to close without specialized medical intervention. |
Seeing it laid out like this makes it clear: these are two completely different problems requiring vastly different approaches.
The impact of these non-healing wounds is staggering. In the United States, they affect roughly 10.5 million Medicare beneficiaries—that’s about one in six elderly individuals. The financial burden is just as massive, with Medicare spending an estimated $22.5 billion each year to manage what many experts have called a silent epidemic. You can read the full research on this public health issue here.
A chronic wound is more than just a break in the skin; it's a complex medical problem where the body's healing signals have gone silent. Restoring those signals requires a targeted approach that goes beyond a simple bandage.
Recognizing these distinctions is the first step toward getting the right care. It also underscores why collaborative models are so critical for tackling these complex cases. You can learn more about the goals of advanced home wound collaborative care and see how modern strategies are making a real difference. The journey from a stalled wound to a healed one begins by figuring out why the process stopped in the first place.
The Hidden Culprits That Stall Wound Healing
To figure out what makes a wound chronic, we have to look past the skin's surface and find the roadblocks stalling the body’s natural repair process. These wounds don't stick around out of stubbornness; they're symptoms of deeper, underlying issues. Three main culprits are usually responsible for turning a simple injury into a long-term battle.
The most common saboteur is poor circulation. Think of your healing process like a massive construction project. Your blood vessels are the highways delivering all the essential materials—oxygen, nutrients, and cellular "workers"—to the job site. When circulation is weak, those supply lines are cut off, and the wound is starved of everything it needs to rebuild.
This problem is almost always tied to other health conditions. For example, peripheral artery disease (PAD) narrows the arteries, while diabetes can damage the tiny blood vessels, creating a physiological drought right where the body needs moisture and nutrients the most.
Sustained Pressure and Constant Irritation
Another major obstacle is sustained pressure. When one part of the body—often over a bony spot like a heel or hip—is under constant pressure, it squeezes the blood vessels shut. It’s just like standing on a garden hose; no water can get through to nourish the plants.
This lack of blood flow robs the tissue of oxygen, causing it to break down and form an ulcer. People with limited mobility are especially vulnerable because they can't shift their weight often enough to let the blood flow back in. To make matters worse, constant friction and shear forces, which stretch and tear the skin, only add to the damage.
It's not just about outside forces, either. Internal conditions are critical. Compromised blood flow, or a lack of proper understanding tissue perfusion and its importance, can bring the healing process to a complete halt.
Unchecked Inflammation and Infection
The last major culprit is a biological standoff caused by infection or chronic inflammation. In a normal healing process, inflammation is a good thing—it’s a temporary stage where the body cleans the wound. But in a chronic wound, the body gets stuck in this phase, and the inflammation starts doing more harm than good.
An infected or overly inflamed wound is like a battlefield where the conflict never ends. The constant fighting prevents any rebuilding, and the body's resources are exhausted just trying to manage the chaos.
Bacteria can create a protective shield around themselves called a biofilm, which makes them incredibly resistant to both your immune system and antibiotics. This persistent microbial presence keeps the wound in a state of high alert, preventing it from ever moving on to the rebuilding phase.
Identifying which of these culprits—or what combination of them—is at play is the essential first step. Only then can we develop a treatment plan that finally clears the roadblock and gets the healing journey back on track.
Identifying Common Types of Chronic Wounds
While the root causes of a chronic wound often boil down to a few key culprits—poor circulation, infection, or relentless pressure—how they show up can look very different from person to person. Think of chronic wounds not as a single problem, but as a family of related issues, each with its own story and distinct profile.
Recognizing the specific type of wound is the first step. More often than not, these wounds are a symptom of a much larger, systemic health issue. That means we aren't just treating a sore; we're managing an underlying condition.
Diabetic Foot Ulcers
For anyone living with diabetes, even a tiny blister or cut on the foot can escalate into a serious health threat. Diabetic foot ulcers are open sores that crop up most often on the bottom of the feet, and they’re a direct consequence of two major diabetic complications: nerve damage (neuropathy) and poor circulation.
Neuropathy is the real troublemaker here. It dulls sensation, so a person might not even feel the initial injury. A small problem can then go unnoticed, festering until it becomes a significant ulcer. These often look like a deep crater surrounded by a border of callused skin.
A diabetic foot ulcer is a stark reminder of how a systemic disease can manifest locally. The lack of sensation and blood flow creates a perfect storm where minor trauma can lead to a non-healing wound that risks infection and even amputation if left untreated.
Venous Leg Ulcers
By far the most common type we see, venous leg ulcers typically appear on the lower leg, somewhere between the knee and the ankle. The underlying cause is venous insufficiency, a condition where the veins in your legs just can't effectively pump blood back up to the heart.
This causes blood to pool in the lower legs, which ramps up the pressure inside the veins. Fluid starts to leak into the surrounding tissues, making the skin fragile, swollen, and discolored—often a telltale reddish-brown. Eventually, the skin breaks down, forming a shallow but often large, irregularly shaped sore that may ooze fluid.
The diagram below breaks down the three main factors that conspire to stall the healing process.
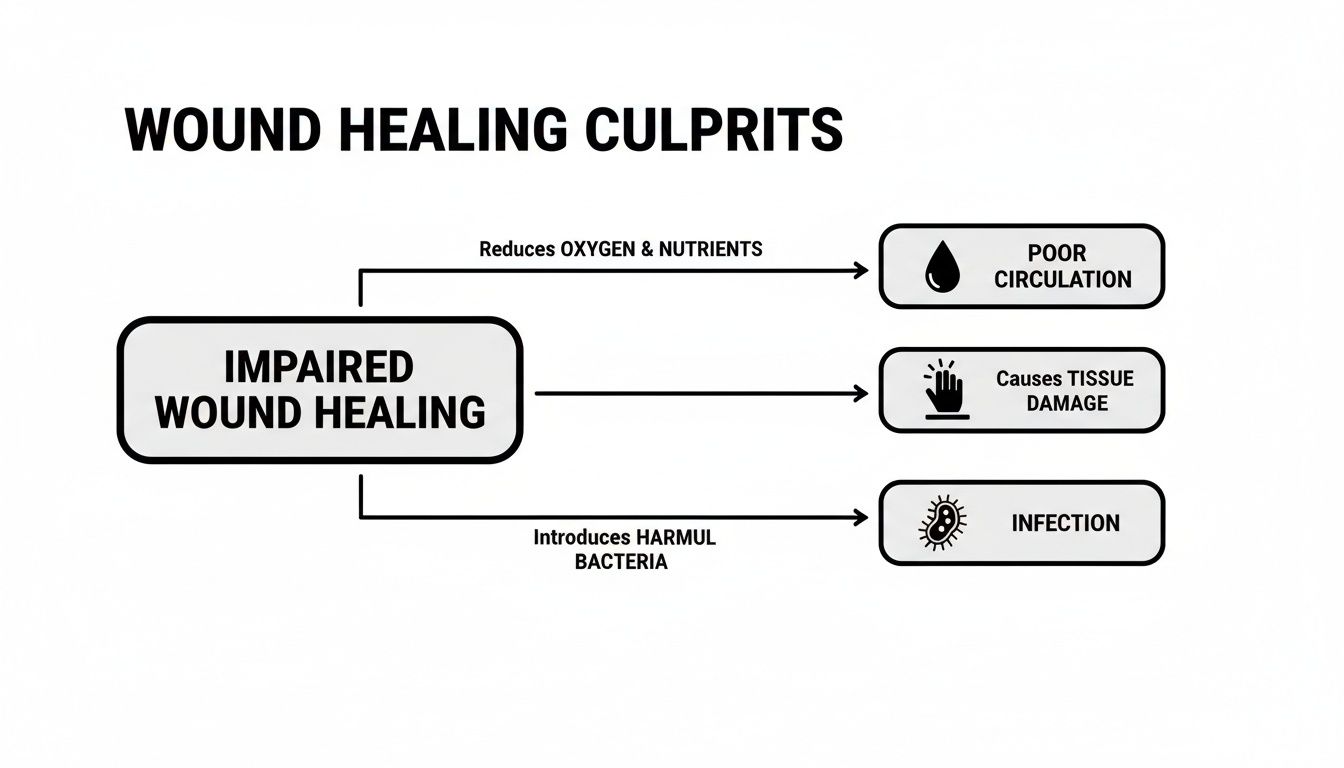
As you can see, poor circulation, sustained tissue damage, and infection create a vicious cycle that keeps a wound from closing.
Arterial Ulcers and Pressure Injuries
On the flip side of venous ulcers, we have arterial ulcers (also called ischemic ulcers). These are caused by the exact opposite problem: not enough oxygen-rich blood is getting to the legs and feet because of blocked arteries.
- Appearance: They have a classic "punched-out" look—deep, circular, and with very well-defined borders. Because of tissue death, the wound bed is often pale or even black. The surrounding skin can feel cool to the touch and may look shiny and hairless.
- Location: You’ll usually find these painful ulcers on the toes, heels, or bony parts of the ankles.
Finally, there are pressure injuries, which you might know as bedsores or decubitus ulcers. They are caused by prolonged, uninterrupted pressure on the skin, which cuts off blood flow and leads to tissue damage. They almost always develop over bony areas like the hips, tailbone, heels, and elbows, particularly in people with limited mobility. The severity can range from a patch of red, unbroken skin to a deep, open wound exposing muscle and bone.
Chronic wounds aren't just a medical issue; they're a massive public health and economic challenge. An estimated 2% of the US population is dealing with a chronic wound, and that figure climbs to nearly 3% for those over 65. The financial burden is staggering. In the US, venous leg ulcers alone cost an estimated $4.94 billion to treat each year. You can discover more insights about the chronic wound care market here.
How Specialists Diagnose a Non-Healing Wound
Figuring out why a wound won’t heal is a lot like detective work. It’s not a quick glance; it’s a full-on investigation to uncover what’s stalling your body’s natural repair process. When you see a specialist, they’re piecing together clues to get to the root of the problem. After all, the only way to fix the wound is to address what’s causing it in the first place.
The whole process kicks off with a detailed conversation. Your provider will want to know your complete medical history—everything from conditions like diabetes or heart disease to the medications you take and your daily habits. They’ll also ask about the wound’s origin story: how it started, how long it’s been there, and what you’ve tried so far.
The Hands-On Examination
Next, the specialist will do a physical examination of the wound and the skin around it. You’d be surprised how much they can learn just by looking and feeling.
- Wound Characteristics: They’ll carefully measure the wound's size and depth. They're also checking for red flags of infection, like a foul odor or redness, and assessing the kind of tissue in the wound bed itself.
- Periwound Skin: The skin surrounding the wound tells its own story. Is it swollen, discolored, or thin and fragile? These signs can point directly to issues like poor circulation.
- Circulation Check: To get a real-time sense of your blood flow, your provider will feel for pulses in your feet and legs.
A proper diagnosis is a systematic process of elimination. The specialist starts with the big picture—your overall health—and gradually narrows down the focus to the specific biological roadblocks preventing your wound from closing.
This initial hands-on assessment helps the specialist form a working theory. To confirm what they suspect, they’ll turn to objective diagnostic tests that give them a crystal-clear picture of what’s happening beneath the surface.
Using Advanced Tools for a Deeper Look
To move from an educated guess to a firm diagnosis, specialists use specific tools to measure how your body is functioning and identify any hidden issues.
One of the most common and vital tests is the Ankle-Brachial Index (ABI). It’s a simple, non-invasive test that compares the blood pressure in your ankle to the pressure in your arm. The result gives a straightforward score that shows how well blood is flowing to your legs and feet, making it an excellent tool for diagnosing peripheral artery disease.
In some cases, a small tissue sample, known as a biopsy, might be needed to check for infection deep within the wound or to rule out other problems. Modern diagnostics have completely changed the game here. For instance, using methods for advanced pathogen detection can rapidly identify the specific bacteria causing an infection. This allows for highly targeted antibiotic treatment, getting you on the right medication much faster than traditional lab cultures ever could.
Modern Treatments That Kickstart Healing
Once a chronic wound is identified and properly staged, the real work begins. We have to shift gears from just managing the problem to actively kickstarting the body's stalled healing engine. Modern wound care isn't about slapping on a bandage and hoping for the best; it's a proactive strategy to clear out the roadblocks that are preventing recovery.
Think of it like trying to revive a neglected garden. You wouldn't just throw seeds on hard, weed-infested soil. First, you have to pull the weeds, aerate the ground, and add the right nutrients. It’s the same with a chronic wound—we have to prepare the wound bed before it can truly start to heal.
Laying the Foundation for Healing
The first, and maybe most critical, step is debridement. This is just a clinical term for the careful removal of any dead, damaged, or infected tissue from the wound. This unhealthy tissue acts like a shield, physically blocking the healthy, healing cells from getting to work and rebuilding.
Next, we focus on choosing the right advanced dressings. These are a world away from the simple gauze pads you might find in a first-aid kit. Modern dressings are engineered to create the perfect microenvironment for healing. They can maintain ideal moisture levels, absorb excess fluid without drying things out, and protect the fragile new tissue from bacteria.
Finally, for many wounds, offloading is non-negotiable. This simply means taking every ounce of pressure off the injured area. For a diabetic foot ulcer, this could mean a special boot or cast designed to redistribute body weight, allowing critical blood flow to reach the wound site and fuel the healing process.
A successful wound care plan is built on these three pillars: a clean wound bed (debridement), a protected and moist environment (dressings), and the removal of physical stress (offloading). Without this solid foundation, even the most powerful therapies will struggle to make a difference.
Advanced Therapies That Accelerate Recovery
With the basics firmly in place, a specialist can bring in more powerful therapies to give the body an extra push. One of the most common and effective is Negative Pressure Wound Therapy (NPWT). This involves placing a specialized foam dressing over the wound, sealing it with a film, and connecting it to a small, portable vacuum pump.
The gentle but constant suction works wonders—it pulls excess fluid away, reduces swelling, and actively encourages the growth of healthy new tissue from the bottom up.
Another game-changer is the use of cellular and tissue-based products. Think of these advanced biologics, like amniotic membrane allografts, as a natural scaffold. They provide the structure and the critical growth factors your own cells need to migrate across the wound and build new skin. This is especially useful for those large, deep, or stubborn wounds that the body just can't seem to bridge on its own.
Overview of Modern Wound Care Therapies
To put it all together, here’s a quick look at how these different therapies fit into a comprehensive treatment strategy. The right tool is chosen for the right job, always with the goal of moving the wound toward closure.
| Treatment Category | Primary Goal | Commonly Used For |
|---|---|---|
| Debridement | Remove non-viable tissue to create a clean wound bed | Wounds with slough, eschar, or signs of infection |
| Advanced Dressings | Maintain a moist, protected healing environment | All chronic wound types, tailored to exudate levels |
| Offloading | Relieve pressure to restore blood flow and prevent re-injury | Diabetic foot ulcers, pressure injuries |
| Negative Pressure Wound Therapy (NPWT) | Reduce edema and stimulate granulation tissue formation | Deep, complex wounds with moderate to heavy exudate |
| Cellular & Tissue-Based Products | Provide a scaffold and growth factors to stimulate healing | Large, non-healing wounds that have stalled |
Ultimately, a specialist will develop a personalized plan, often drawing on established frameworks like these practical treatment plan examples to structure the care.
These interventions show that healing a chronic wound isn't about waiting—it's about acting with a precise, scientific strategy. You can learn more about the specific advanced treatment options that combine these methods to deliver targeted, effective care right where it's needed.
Got Questions About Chronic Wounds? We Have Answers.
Walking the path of chronic wound care can feel confusing, and it's completely normal to have questions. We've gathered some of the most common concerns we hear from patients and their families, offering clear, straightforward answers to guide you on your healing journey.
How Long Does It Take for a Chronic Wound to Heal?
This is one of the first questions we get, and the honest answer is: there's no magic number. A wound's healing timeline is as unique as the person it's on. It really hinges on what caused the wound in the first place, your overall health, and how closely you can stick to the treatment plan.
The real goal isn't speed, it's steady progress.
Some wounds show amazing improvement within a few months of dedicated care. Others might take a year, or even longer, to fully close. The most important thing is tackling the root cause—like getting blood sugar under control for a diabetic ulcer or boosting circulation for an arterial ulcer. That's what truly paves the way for healing.
When Should I See a Wound Care Specialist?
If you have any wound that hasn't shown clear signs of healing within two to four weeks, it's time to call in an expert. Don't wait and hope for the best; early intervention is key.
There are also a few red flags that mean you should seek help right away:
- Pain that’s getting worse: Healing shouldn't become more painful over time.
- A bad smell: A persistent, foul odor is a major sign of infection.
- A lot of drainage: An unusual amount of fluid, especially if it's thick or has changed color, needs to be checked out.
- Redness spreading outward: If the skin around the wound is getting redder or feels warm, that can signal a spreading infection.
And if you're managing a condition like diabetes, peripheral artery disease, or venous insufficiency, our advice is to see a specialist for any new wound on your feet or legs. These areas are at high risk, and getting an expert involved from day one can make all the difference.
You should not have to "tough out" significant pain from a chronic wound. It's often a sign of a deeper issue, like infection or poor blood flow, that a specialist needs to address as part of your overall treatment plan.
Can My Diet and Lifestyle Really Affect Wound Healing?
Absolutely. Think of it this way: your body is a construction site, and the wound is a major repair project. What you eat and how you live are the supplies and the workforce.
Proper nutrition provides the essential building blocks for your body to create new skin and blood vessels. A balanced diet should be rich in:
- Protein: This is the literal raw material for tissue repair.
- Vitamins: Vitamin C and Vitamin A are particularly critical for the healing process.
- Minerals: Zinc is a key player in helping new cells grow and repair the damage.
Lifestyle choices are just as crucial. Smoking, for example, constricts your blood vessels and chokes off the blood flow that healing tissue desperately needs. It can bring the entire process to a grinding halt. Quitting is one of the single most powerful things you can do to help your wound heal.
The same goes for managing your other health conditions. Diligently controlling your blood sugar if you have diabetes or consistently elevating your legs for venous ulcers aren't just suggestions—they are active, non-negotiable parts of your treatment plan that directly support the work your wound care team is doing.
At Specialty Wound Care, we don't just treat the wound; we investigate the "why" behind it. By combining advanced diagnostics with personalized treatment plans, we get to the root cause of why a wound isn't healing. If you or someone you care about is struggling with a stubborn wound, we’re here to clear the roadblocks and get you firmly on the path to recovery. Learn how our expert team can support you by visiting https://specialtywoundcare.com.
