
A Guide to Wound Care Billing and Coding
Let’s be honest, successful wound care billing isn't just about codes. It all starts with a bulletproof foundation of clinical documentation. This is where you connect your clinical expertise directly to your practice's financial health.
Think of your patient chart as the ultimate storyteller. It has to paint a vivid, detailed picture for the payer, leaving zero doubt about the medical necessity of the care you provided. Without this detailed narrative, even the most accurately selected codes can get kicked back.
Payers operate on a simple principle: if it wasn't documented, it wasn't done. This is why seeing documentation as just another administrative chore is a critical, and often costly, mistake. Instead, it should be your first and best line of defense against claim rejections and audits.
Build a Bulletproof Foundation with Documentation
To create documentation that can withstand scrutiny, every single note has to contain specific, objective details that justify your treatment choices. Vague descriptions like "wound improving" just won't cut it. Your notes must be a precise log of the wound's status and your interventions.
The Anatomy of a Defensible Wound Care Note
Here are the essential elements your notes must include every time:
- Precise Measurements: Document the length, width, and depth in centimeters at every visit. This is how you show progression or regression over time.
- Tissue Type and Percentage: Get specific about the amount of granulation, slough, or eschar. For example, "Wound bed is 70% granulation tissue, 30% yellow slough."
- Drainage Details: Describe the amount (scant, moderate, copious), color, and any odor from the exudate.
- Periwound Skin Condition: Note the status of the surrounding skin. Are you seeing maceration, erythema, or induration? Write it down.
- Signs of Infection: Clearly record any clinical signs of infection, such as increased pain, warmth, or purulent drainage.
- Patient’s Response to Treatment: Detail how the patient is tolerating the current plan and any adjustments you made based on their response.
Viewing your documentation as a chore is a critical financial error. Instead, see it as your best defense against audits and denials, directly connecting your clinical skill to your practice's financial health.
A Real-World Scenario: Diabetic Foot Ulcer
Imagine a patient with a chronic diabetic foot ulcer. A weak note might just say, "Patient seen for DFU. Debrided wound. Dressing applied." This tells the payer next to nothing and provides no real justification for the service.
Now, here's what a strong, defensible note looks like. It tells the whole story:
"Patient presents for follow-up of a 3.5 cm x 2.8 cm x 0.4 cm plantar ulcer on the right foot. Wound bed contains 60% adherent yellow slough and 40% pale granulation tissue with moderate serosanguinous drainage. Periwound shows 1 cm erythema. Sharp excisional debridement was performed to remove all non-viable tissue down to the subcutaneous layer. Post-debridement measurements are 3.6 cm x 3.0 cm x 0.5 cm with a 100% granular base."
See the difference? This level of detail proves the medical necessity for the debridement (CPT 11042) and justifies the E/M service. If you're looking to elevate your team's skills, exploring structured training can provide invaluable workflows and templates. You can learn more in our guide on wound care training and documentation: https://specialtywoundcare.com/training-documentation/
And remember, ensuring all patient records are handled securely is non-negotiable. For a deep dive into making sure your documentation and transmission methods meet regulatory standards, this guide on HIPAA compliant faxing in healthcare is an invaluable resource.
The financial impact of getting this wrong is huge. In 2025, coding and documentation errors are a major source of lost revenue, with CMS reporting that these mistakes lead to 7–10% of all claim rejections annually. That statistic alone highlights the high stakes in a field where services range from simple dressing changes to complex debridements and advanced allografts.
Select the Right CPT and HCPCS Codes
Once your documentation is ironclad, the next step is to translate that clinical story into the right CPT and HCPCS codes. This is a common stumbling block for many practices. Even a minor coding mistake can lead to denied claims, lost revenue, and unwanted attention from auditors.
Think of it this way: CPT and HCPCS codes are the language payers understand. Choosing the correct one isn't just a suggestion; it's essential for getting paid accurately for the work you do. This means digging into the subtle but critical differences between similar code sets to find the one that perfectly matches the service you documented.
Distinguishing Between Debridement Codes
Debridement coding is probably one of the trickiest areas in wound care. Payers scrutinize these codes, so you absolutely have to know the difference between the two main categories. It all comes down to the method used and how deep you go.
To help clear things up, here’s a quick comparison of the debridement code families.
Debridement Code Selection Guide: Selective vs. Non-Selective
| Code Type | CPT Codes | Method Used | Basis for Coding | Key Documentation Requirement |
|---|---|---|---|---|
| Selective | 97597 / 97598 | Sharp instruments, high-pressure water jets to remove specific, non-viable tissue. No anesthesia required. | Surface area of the wound(s) in square centimeters. | Detailed description of the non-viable tissue removed (e.g., slough, fibrin). |
| Excisional / Non-Selective | 11042 – 11047 | Surgical excision with instruments like scalpels or curettes to remove tissue down to a viable base. | Deepest layer of tissue removed (e.g., subcutaneous, muscle, bone) and surface area. | Clear identification of the deepest tissue layer cut away and removed. |
The most important thing to remember is that you can’t bill for both types of debridement on the same wound during the same visit. Your notes have to paint a clear picture that justifies the code you picked.
Key Takeaway: Always code debridement based on the deepest layer of tissue removed, not the deepest layer visible in the wound bed. If a wound extends to the bone but you only debride subcutaneous tissue, you must use the code for subcutaneous tissue (11042).
Coding for Negative Pressure Wound Therapy
Negative Pressure Wound Therapy (NPWT) is a go-to treatment in wound care, and its coding is very specific. The main CPT codes you'll use are 97605-97608. Picking the right one boils down to two things: the wound size and whether the device is considered durable medical equipment (DME).
- CPT 97605: Use this for a total wound surface area of 50 square centimeters or less.
- CPT 97606: This is for a total wound surface area greater than 50 square centimeters.
- CPT 97607 & 97608: These codes are for home care settings where the therapy device is disposable and not classified as DME.
Accurate wound measurements are non-negotiable here—they are your proof for the code you've chosen. Also, keep in mind that applying a multi-layer compression system, which often goes hand-in-hand with NPWT, is a separate service. You might be able to bill for it with its own code if it’s medically necessary.
This simple decision tree drives home the financial impact of getting your documentation right.
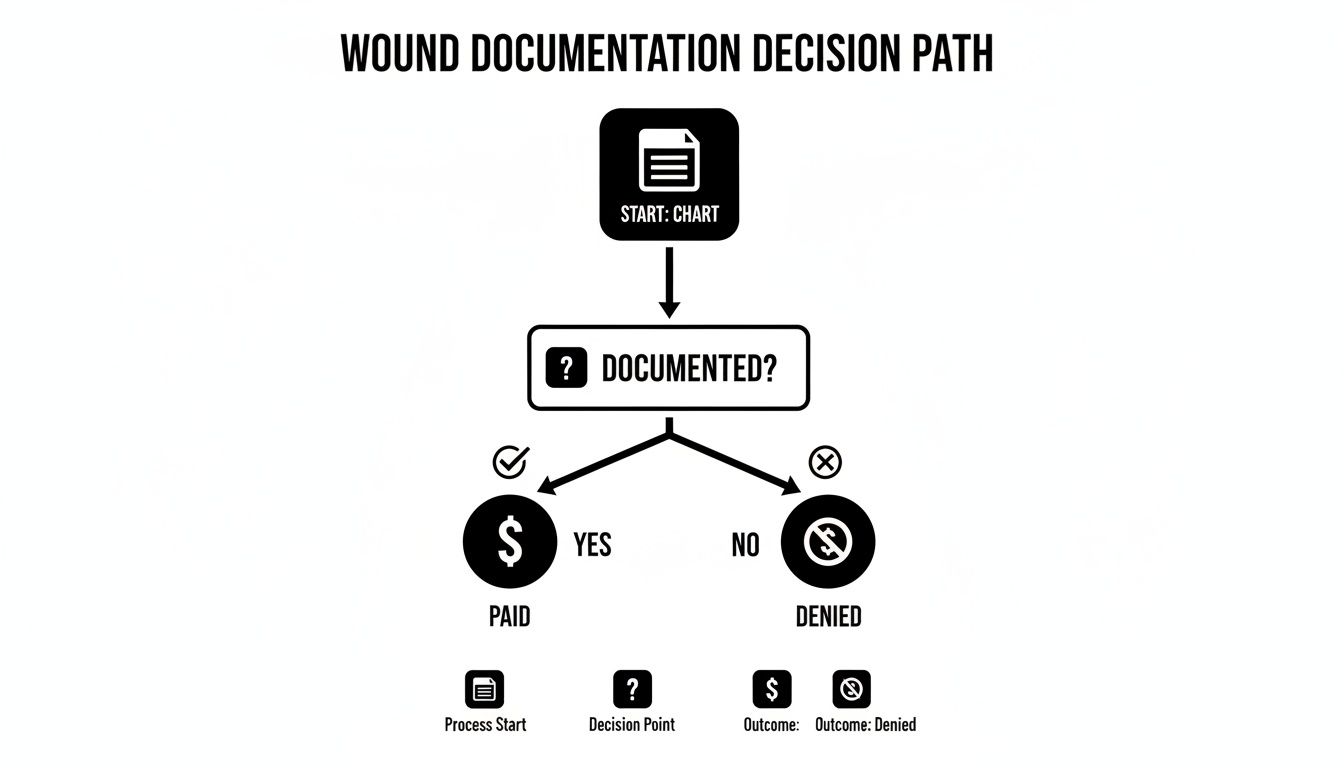
As you can see, a documented service gets paid. A service without documentation gets denied. It’s a straightforward but powerful reality in our field.
Billing for Skin Substitutes and E/M Services
Advanced treatments, like applying skin substitutes or cellular and/or tissue-based products (CTPs), introduce another layer of coding complexity. These are usually billed with HCPCS codes that change depending on the exact product used (think high-cost vs. low-cost grafts). You have to document the product name, the size, how much was applied, and how much was wasted.
On top of that, many wound care visits also include an Evaluation and Management (E/M) service. You can bill an E/M code on the same day as a procedure like debridement, but only if the E/M is a significant, separately identifiable service. This means you need to append modifier -25 and have documentation that clearly separates the thinking and decision-making (the E/M) from the hands-on procedure. For example, if a patient is scheduled for debridement but also presents with a new, unrelated issue that you have to assess and manage, that E/M work is likely billable.
For clinicians looking to integrate more of these therapies, exploring the advanced treatment options by Primus Specialty Wound Care can offer valuable insight. Getting these codes right ensures your practice is compensated fairly for the complexity and value of the care you provide.
Tell the Full Story with ICD-10-CM Diagnosis Codes
Let's get one thing straight: an accurate diagnosis code does way more than just identify a wound. It tells the payer the entire patient story, justifying every single service you provide and proving why your care is medically necessary.
Think of it this way. Your CPT codes explain what you did, but the ICD-10-CM codes explain why you did it. Mastering the ICD-10-CM code set for wound care isn't just about checking a box for compliance—it's about painting a crystal-clear clinical picture that gets you paid.
Using a generic ulcer code is like telling a mechanic "there's a problem with the car." It’s useless. But a highly specific code is like saying, "there's a slow leak in the front-left tire from a nail puncture." Now the mechanic knows exactly what’s needed. Vague coding forces payers to guess, and that guesswork almost always leads to denials.
For chronic, non-healing ulcers, coding to the highest level of specificity is absolutely non-negotiable. You have to capture every last detail about that wound and the patient's overall health.
Go Beyond the Basic Wound Diagnosis
To really build that clinical narrative, your diagnosis coding has to be multi-layered. Just coding for "pressure ulcer" won't cut it. Payers need to know the location, the severity, and all the underlying factors that are making the wound so stubborn.
Here are the critical details that need to be reflected in your ICD-10-CM code selection every time:
- Anatomical Location and Laterality: Is the ulcer on the right heel or the left ankle? Specificity is everything. Use the codes that pinpoint the exact site.
- Pressure Ulcer Staging: For pressure injuries, you must include the stage. A Stage 4 ulcer demands a completely different level of care than a Stage 1, and your coding has to show that.
- Underlying Conditions: You have to link the wound to its root cause. If a patient has a diabetic foot ulcer, you must use a code that connects the diabetes to the foot complication, like E11.621 (Type 2 diabetes mellitus with foot ulcer).
- Associated Comorbidities: Does the patient also have peripheral arterial disease (PAD) or venous insufficiency? These conditions directly sabotage healing and justify more intensive treatments. You need to code them as secondary diagnoses.
Precise ICD-10 coding is your most powerful tool for demonstrating medical necessity. It connects the wound to the patient's systemic health, building an undeniable case for the care you provide and improving quality metrics in a value-based care world.
A Home Health Case Study
Let's walk through a common scenario to see how this all comes together. A home health nurse is treating an 82-year-old bed-bound patient with a pressure ulcer.
A lazy or inexperienced coder might just use L89.159 (Pressure ulcer of sacral region, unspecified stage). This code is a red flag. It’s incomplete and practically begs for a denial or a request for more information because it lacks any real detail.
A robust, defensible coding approach tells the complete story:
- Primary Diagnosis: L89.154 (Pressure ulcer of sacral region, Stage 4). Right away, this establishes the severity and location of the main problem.
- Secondary Diagnosis: I70.211 (Atherosclerosis of native arteries of extremities with intermittent claudication, right leg). This explains that poor circulation (PAD) is a major complicating factor, justifying more advanced interventions.
- Additional Diagnoses: I10 (Essential hypertension) and E78.5 (Hyperlipidemia). These comorbidities create a much fuller picture of the patient's overall health, which absolutely influences the plan of care.
This combination of codes provides a comprehensive clinical snapshot. It tells the payer this isn't just some simple wound; it's a severe, Stage 4 pressure injury on a patient with compromised circulation and other chronic illnesses. This is the level of detail payers need to see to approve claims for services like frequent debridement or advanced wound dressings without a fight. Getting this right is crucial for your financial viability.
Unlock Reimbursement with the Right Modifiers
Think of modifiers as the essential fine print on your wound care claims. While CPT and ICD-10 codes tell payers what you did and why you did it, modifiers add that crucial bit of context. Get them right, and you have a paid claim. Get them wrong, and you're looking at an immediate denial.
These simple two-digit codes are your way of clarifying special circumstances, preventing incorrect bundling, and ultimately, defending your reimbursement. Honestly, ignoring modifiers in wound care is like sending a text without any punctuation—the core message might be there, but the real meaning gets lost. For a payer, that missing context often signals an unbillable service, leading to rejections that just drain your time and resources.
Modifier 25 for Same-Day Services
Let’s start with a common one that trips people up: Modifier 25. You'll need to append this to an Evaluation and Management (E/M) code when you perform a significant, separately identifiable E/M service on the same day as another procedure.
Here’s a real-world scenario. A patient comes in for a scheduled debridement of a venous leg ulcer. During that visit, they mention a new, painful lesion that’s popped up on their other foot. To address it, you have to perform a separate exam, dig into their history, and go through the medical decision-making process for this brand-new problem.
- The Procedure: The scheduled debridement (e.g., CPT 97597).
- The E/M Service: The assessment of the new lesion, which is completely distinct from the routine pre-service work for the debridement.
In this case, you’d bill the appropriate E/M code (like 99213) with Modifier 25 attached. This signals to the payer that your E/M work went above and beyond the standard care baked into the debridement procedure. Without it, they'll almost certainly bundle the E/M service into the procedure payment, leaving you uncompensated for that extra work.
Using Modifier 59 to Unbundle Procedures
Another workhorse in wound care is Modifier 59, which identifies a "Distinct Procedural Service." This is your go-to when you need to tell a payer that two procedures done on the same day aren't related and should each be paid separately. It’s often considered the modifier of last resort when a more specific one doesn't fit the bill.
A classic example is treating multiple, distinct wounds. Imagine you perform an excisional debridement (CPT 11042) on a sacral pressure ulcer and a selective debridement (CPT 97597) on a diabetic foot ulcer—all during the same visit.
Since CPT codes 11042 and 97597 aren't typically billed together for the same wound, you absolutely must use Modifier 59 on CPT 97597. This clearly indicates it was performed on a different anatomical site, stopping the payer's automated system from flagging it as a duplicate service.
The Critical Role of the KX Modifier
When you’re dealing with services that have frequency limits, the KX modifier is your key to proving medical necessity. Payers like Medicare often cap how many debridements a patient can receive in a certain timeframe. The KX modifier is your official attestation that the documentation in the patient’s chart fully supports the need to exceed those limits.
Think of a patient with a rapidly deteriorating wound that requires debridement more often than the local coverage determination (LCD) usually allows. By adding the KX modifier to the debridement code, you are certifying two things:
- The service meets the specific coverage criteria outlined in the payer's policy.
- You have comprehensive documentation on file ready to prove it if they ask.
Be warned: using this modifier without rock-solid documentation is a huge compliance risk. Your notes must paint an unmistakable picture of why the additional service was not just helpful, but absolutely essential to the patient's care plan.
To help you keep these straight, here's a quick-reference guide to some of the most essential modifiers you'll encounter in wound care. It's a handy cheat sheet to ensure you're applying them correctly and telling the full story on your claims.
Essential Wound Care Modifiers and Their Applications
| Modifier | Description | When to Use in Wound Care (Example) |
|---|---|---|
| 25 | Significant, Separately Identifiable E/M Service by the Same Physician on the Same Day of the Procedure or Other Service | A patient is scheduled for a debridement. During the visit, they present a new, unrelated complaint (e.g., a suspicious skin lesion) that requires a separate workup. You would append Modifier 25 to the E/M code. |
| 59 | Distinct Procedural Service | You perform a debridement on a right foot ulcer (CPT 97597) and apply a skin substitute to a left leg ulcer (CPT 15275) in the same session. You would use Modifier 59 on the second procedure code to show it was a separate site. |
| KX | Requirements Specified in the Medical Policy Have Been Met | A patient with a severe, rapidly necrotizing wound requires debridements more frequently than the payer's policy typically allows. Appending the KX modifier attests that documentation supports the medical necessity for the increased frequency. |
| 76 | Repeat Procedure or Service by Same Physician or Other Qualified Health Care Professional | The same physician has to repeat an unplanned debridement on the same wound later in the same day due to sudden, severe necrosis. Modifier 76 indicates it is not a duplicate charge. |
| LT/RT | Left Side / Right Side | Used to specify which side of the body a procedure was performed on, which is critical for clarity when treating bilateral wounds. For example, billing for debridement of a wound on the right heel (using RT). |
Mastering these modifiers isn't just about administrative box-ticking; it's a fundamental skill for running a financially healthy wound care practice. Correctly applying them ensures you are properly compensated for the vital, and often complex, work you do.
Navigate Payer Policies and Overcome Denials
You can nail the CPT, HCPCS, and ICD-10 codes every single time, but that’s only half the battle. Let’s be real—perfect coding doesn’t guarantee payment if your claims don’t line up with the tangled web of rules set by each payer.
This is where you have to get proactive.
Think of every payer, from a Medicare Administrative Contractor (MAC) to a commercial insurer, as having its own unique rulebook. These are often called Local Coverage Determinations (LCDs) for Medicare or just clinical policies for private payers. They spell out exactly what they consider medically necessary, how often a service can be done, and what proof they need. Ignoring them is just asking for a denial.
Unpacking Common Denial Reasons
Those denial letters can feel cryptic, but after a while, you start to see the patterns. Most rejections in wound care boil down to a handful of common culprits. Getting familiar with them is the first step toward stopping them before they start.
- Lack of Medical Necessity: This is the big one. The payer simply wasn't convinced the service was reasonable and necessary based on the documentation you sent.
- Missing Prior Authorization: Many advanced treatments, like skin substitutes or hyperbaric oxygen therapy, require a green light before you proceed. Skipping this step leads to an automatic denial that’s almost impossible to reverse.
- Exceeding Frequency Limits: Payers often put a cap on how many times a service, like debridement, can be performed in a certain timeframe. Bill for more without a solid justification (like the KX modifier), and you’ll trigger a rejection.
- Incorrect Bundling: This happens when you bill for something the payer considers part of a larger, primary procedure. A classic example is trying to bill separately for applying an Unna boot on the same day as a debridement.
A denied claim isn't just a one-time financial loss; it's a data point. Use it to identify weaknesses in your documentation or billing workflow so you can fix the root cause and prevent similar denials in the future.
This landscape is constantly shifting. The introduction of over 420 CPT code updates in 2025, including 270 new codes, is reshaping wound care billing. These changes, effective alongside 252 new ICD-10-CM codes, demand rigorous training to capture wound specifics—essential for codes like E11.621 for diabetic foot ulcers. You can learn more about these upcoming coding and compliance changes to stay ahead.
Crafting a Compelling Appeal Letter
When a denial inevitably lands on your desk, a well-written appeal is your best shot at getting paid. A weak appeal that just says "we disagree" is a waste of time. A strong one builds a logical, evidence-based case that makes it easy for the reviewer to say yes.
Let's say a claim for excisional debridement (CPT 11043) was denied for "lack of medical necessity." Here’s how to build an appeal that works:
- Get Straight to the Point: Start with a clear introduction. State the patient's name, the claim number, and the specific service being appealed. No fluff.
- Paint the Clinical Picture: Briefly summarize the patient's condition and the wound's history. Explain why other conservative treatments didn't work. This sets the stage and provides crucial context.
- Use Their Own Rules Against Them: This is a powerful move. Directly quote the section of the payer's own medical policy or LCD that supports the service you provided. For example, "Per your LCD L33614, excisional debridement is considered medically necessary for wounds with non-viable tissue."
- Connect the Dots: This is where you win or lose the appeal. Systematically pull direct quotes from your clinical notes that match the policy requirements you just cited. For instance, "The progress note from [Date] documents '75% adherent yellow slough with necrotic edges,' which meets the criteria for non-viable tissue requiring removal."
- Show, Don't Just Tell: Don't just send the letter. Attach copies of the relevant progress notes with the key phrases highlighted. Include clear wound photos showing the non-viable tissue and any other supporting lab results.
- Close Professionally: End with a polite request for them to re-evaluate the claim for payment based on the evidence you’ve laid out.
To really get ahead of denials, many practices are finding that automated claims processing can be a huge help. It’s a proactive approach that gives your practice the tools to prevent denials from happening in the first place, not just react to them after the fact.
Common Questions on Wound Care Billing
Even when you feel you’ve mastered the fundamentals, certain situations in wound care billing can make the most seasoned pros second-guess themselves. Let's walk through some of the tricky questions we see pop up in daily practice and give you direct answers you can use on your very next claim.
These are the exact scenarios where practices often lose revenue or accidentally take compliance risks. Getting them right is non-negotiable for a healthy revenue cycle.
Can We Bill for an E/M Service During a Post-Operative Period?
This one comes up all the time. The short answer is yes, but you have to be very careful and use Modifier 24. This modifier flags an "Unrelated Evaluation and Management Service by the Same Physician or Other Qualified Health Care Professional During a Postoperative Period."
Think of it this way: a patient is in their 90-day global period after surgery on their right leg. They come in for a scheduled follow-up but also point out a new problem—an infected cyst on their back. The E/M service you perform for that cyst is completely separate and billable with Modifier 24. Why? Because it has absolutely nothing to do with the original surgery.
Key Takeaway: You can't use Modifier 24 for anything related to the surgery itself. That includes managing complications like a surgical site infection. All of that work is already bundled into the global surgery payment.
How Do We Code Debridement for Multiple Wounds?
Coding multiple wounds hinges entirely on the depth of debridement. The rules here are straightforward, but you have to follow them to the letter to avoid bundling errors and denials.
-
Same Depth: If you debride multiple wounds to the same tissue depth (say, all are subcutaneous), you need to add up the surface area of all the wounds. Then, you report that total using a single CPT code series (like 11042 for the first 20 sq cm and +11045 for each additional area).
-
Different Depths: This is where it gets more granular. If the wounds are debrided to different depths—one down to muscle and another to bone—you must code each one separately. Each wound gets its own primary CPT code based on its specific depth and size.
Mixing these two scenarios is one of the most common mistakes we see, and it almost always results in a denial.
Is It Possible to Bill for a Dressing Change?
In most cases, no. A routine dressing change is considered part of the E/M visit or post-op care. Payers just assume the work and supplies for a standard change are baked into the payment for the main service.
There is an exception, though. If the dressing change is unusually complex and involves procedural work—like meticulously removing embedded, non-viable tissue—it might qualify as a form of debridement. In that case, you could potentially use a code like 97597. Just be warned: your documentation has to be impeccable, clearly describing the skilled work you performed that went far beyond a simple swap of gauze.
For more detailed answers to specific scenarios, you can always check out our comprehensive wound care billing FAQs.
Can an Unna Boot Application Be Billed with Debridement?
Here’s another classic bundling trap. If you perform a debridement and then apply an Unna boot (CPT 29580) to the same wound in the same visit, payers will almost certainly only pay for the debridement. The Unna boot is seen as an integral part of that wound care service.
The only way you can bill for both is if the Unna boot is applied to a completely separate and unrelated wound, or if it's the only procedure you perform during that visit.