
A Clinicians Guide to Wound Debridement Techniques
Wound debridement isn't just a procedure; it's the fundamental first step toward healing. Think of it as clearing a construction site before laying a new foundation. We’re removing all the dead, damaged, or infected tissue from a wound so the body’s own healing mechanisms can finally get to work.
By clearing out this biological debris, debridement helps reduce infection risk and perfectly prepares the wound for advanced therapies. Without a clean wound bed, even the most advanced treatments will struggle to be effective.
The Evolution of Wound Debridement

The idea of cleaning a wound to help it heal is as old as medicine itself, refined over thousands of years through sheer necessity. To really get why we use today’s specific debridement techniques, it helps to look back at where it all started. This journey from simple wound washing to precise, evidence-based protocols has always been driven by one goal: preparing the wound for a successful recovery.
It’s like trying to grow a garden in soil choked with weeds and rocks. No amount of water or fertilizer will help if the seeds can't reach fertile ground. A wound filled with non-viable tissue is exactly the same. Early healers knew this instinctively and developed methods to clear the "soil" of the wound bed.
Ancient Roots of Wound Care
The practice of cleaning wounds goes back over 5,000 years. Around 3000 BCE, the Sumerians were already documenting detailed wound treatments, creating plasters from things like beer, turpentine, and pine resin. For them, beer wasn't just for drinking; they had 19 different types specifically for healing.
The ancient Egyptians took things a step further, creating adhesive bandages and using honey-grease-lint plasters. The honey was a powerful antibacterial agent, and the lint helped draw fluid away from the wound—one of the earliest systematic approaches to cleaning and managing the wound environment. You can learn more about how surprisingly effective these ancient medical practices were.
“The fundamental principle of wound debridement—removing barriers to allow healing—has remained constant through history. What has changed is our understanding of the science behind it and the precision of our tools.”
This history is important. It shows that controlling the wound environment has always been at the heart of patient care, setting the stage for the scientific breakthroughs that would follow.
The Battlefield Forges Modern Debridement
The real leap from ancient art to modern science happened on the battlefield, where severe trauma created an urgent need for better solutions. Through the 19th century, surgeons started to formalize the removal of dead tissue, but high infection rates meant outcomes were still grim.
Then came pioneers like Carl von Reyher during the Russo-Turkish War. He didn't just cut away damaged tissue; he combined it with the antiseptic principles of Joseph Lister. This dual approach—aggressively cleaning the wound and preventing new bacterial growth—was a game-changer.
By applying this method, Reyher saw a stunning 43% drop in mortality rates compared to earlier battlefield treatments. His success proved just how critical aggressive debridement was, cementing its place as a standard of care in both military and civilian medicine. This history is a powerful reminder that today's debridement techniques were forged through centuries of trial, error, and life-saving innovation.
Why Debridement Is Critical for Wound Healing

To grasp why wound debridement is so fundamental, think of a neglected garden. It’s choked with weeds, dead plants, and debris. No matter how much you fertilize or water, new life can't take root until you clear the soil. A chronic wound is much the same.
A wound bed covered in non-viable tissue is a wound that's stuck. This buildup of necrotic tissue, slough, or eschar creates a physical wall, stopping healthy new cells from migrating across the surface to close the gap. But it's not just a passive barrier; it actively sabotages the healing process.
Removing the Barriers to Healing
The main goal of any debridement technique is to get rid of these roadblocks. Necrotic tissue isn’t just dead weight—it’s a five-star buffet for bacteria. This non-viable material provides an endless food source for pathogens, helping them multiply and form stubborn communities called biofilms.
Biofilms are a major problem in wound care. They create a slimy, protective shield that makes bacteria incredibly resistant to both the body’s immune defenses and antibiotics. This persistent bacterial presence, or high bioburden, locks the wound in a state of chronic inflammation, preventing it from ever moving forward into the rebuilding phases of healing.
By physically removing the dead tissue and biofilm, debridement breaks the bacterial stronghold, dials down inflammation, and essentially hits the "reset" button on the wound. This clears the way for the body’s natural healing cascade to finally get to work.
This is why we see debridement as an active, therapeutic procedure, not just a simple cleaning step.
Enabling Accurate Assessment and Treatment
Another crucial role of debridement is that it allows clinicians to see what’s really going on under the surface. A wound buried under thick eschar is like a house with the curtains drawn—you have no idea what’s happening inside.
Clearing away the surface debris is the only way to:
- Accurately measure the wound: Clinicians can finally determine the true depth, width, and overall volume.
- Visualize underlying structures: It reveals if any bone, tendon, or other vital tissues are exposed and need protection.
- Assess tissue viability: Debridement makes it possible to distinguish healthy, pink granulation tissue from unhealthy, compromised tissue.
This clear view is absolutely vital for staging the wound correctly and choosing the right treatment path. Without it, clinicians are essentially flying blind. Accurate assessment also depends on knowing which specific pathogens are present, and you can learn more about how advanced pathogen detection can guide treatment by providing fast, precise answers.
Ultimately, debridement prepares the wound bed for everything that comes next. Whether the plan involves a simple dressing or an advanced therapy like a skin graft, success hinges on a clean, healthy, and receptive wound environment. Debridement is the essential first step that makes all other care possible, converting a chronic, stalled wound into an acute wound that is ready to heal.
Exploring the Five Types of Wound Debridement
Wound debridement isn't a one-size-fits-all procedure. It’s actually a spectrum of specialized techniques, and knowing which one to use is a lot like a skilled tradesperson choosing the right tool for the job. You wouldn't use a sledgehammer where a fine-tipped brush is needed. The best approach depends entirely on the wound's condition, the patient's overall health, and the clinical goals we're trying to achieve.
The five primary methods—surgical, enzymatic, autolytic, mechanical, and biological—each offer a unique way to clear the wound bed. Let's break down how they work and when to use them.
Surgical and Sharp Debridement: The Gold Standard for Speed
When speed is critical, surgical and sharp debridement are the go-to methods. These are often seen as the most aggressive options, where a qualified clinician uses sterile instruments like a scalpel, curette, or scissors to physically cut away dead or infected tissue.
Think of it like a sculptor carefully chipping away stone to reveal the healthy form underneath. A clinician does the same, precisely removing tough eschar and necrotic debris to expose the healthy, bleeding granulation tissue that signals a viable wound bed. This technique is invaluable for clearing large amounts of devitalized tissue or when an infection is spreading fast.
Its roots trace back to military medicine, where quick, decisive action saved lives. The term was popularized by Carl von Reyher in the late 19th century, whose battlefield work transformed medical practice. By combining debridement with antiseptics, he achieved a staggering 43% drop in mortality rates—a landmark achievement that proved the power of aggressive wound cleaning. That legacy continues today, with sharp debridement used in over 70% of surgical cases, making it a cornerstone of modern wound care. You can learn more about the historical impact of debridement on patient outcomes in medical literature.
Enzymatic Debridement: Dissolving Debris Chemically
Enzymatic debridement takes a chemical approach. Instead of cutting, it uses prescribed ointments or solutions that contain enzymes to break down and liquefy necrotic tissue. The most common enzyme is collagenase, which specifically targets and digests the collagen fibers that anchor dead tissue to the wound bed.
Because it leaves healthy tissue alone, this method is far more selective than some mechanical options. It's a great choice for patients who can't tolerate a surgical procedure or for those in long-term care where daily application is more practical. The trade-off is time; it's a slow and steady process that requires patience and consistency.
Key Takeaway: Enzymatic debridement shines when a slower, more selective, and less painful approach is needed for wounds with moderate necrotic tissue. It's often used to prepare a wound for other methods or as a maintenance therapy.
Autolytic Debridement: Harnessing the Body's Own Power
Of all the methods, autolytic debridement is the most natural and gentle. It works by creating a moist wound environment, which lets the body's own enzymes and white blood cells (macrophages) do the work of breaking down and digesting devitalized tissue.
We achieve this by applying moisture-retentive dressings, such as:
- Hydrocolloids: These form a gel over the wound, trapping moisture.
- Hydrogels: These donate moisture to dry wounds, kicking off the autolytic process.
- Transparent films: These trap the wound's own fluid, letting endogenous enzymes work their magic.
Because it leans on the body's innate healing capacity, autolytic debridement is incredibly selective and typically painless. It's perfect for patients with minor to moderate amounts of non-viable tissue who have a healthy immune system and good circulation. The only real downside is that it's the slowest of all debridement techniques.
Mechanical Debridement: Physical Force for Removal
Mechanical debridement uses physical force to remove debris from the wound surface, but it's often non-selective. This category covers several methods, all of which use some form of force to dislodge and clear away contaminants.
One of the oldest forms is wet-to-dry dressings. A moist gauze is placed in the wound, allowed to dry, and then pulled away, taking dead tissue with it. While it can be effective, this method is often painful and can accidentally remove healthy granulation tissue along with the necrotic debris.
Other mechanical methods include:
- Wound Irrigation: Using a pressurized stream of saline to flush out loose debris.
- Hydrotherapy (Whirlpool): Submerging the area in moving water to soften and wash away dead tissue.
- Pulsed Lavage: A system that delivers a pressurized, pulsed stream of fluid combined with suction to remove the liquid and debris.
Because of the risk of harming healthy tissue, older methods like wet-to-dry dressings are falling out of favor, replaced by more selective alternatives.
Biological Debridement: Nature's Most Precise Surgeons
Biological debridement, better known as larval therapy or maggot debridement therapy (MDT), might sound unsettling, but it’s an incredibly precise technique. It uses medical-grade, sterile larvae of the green bottle fly. These tiny organisms are masters of precision, consuming only necrotic tissue and bacteria while leaving healthy tissue completely untouched.
The larvae work in three powerful ways:
- They secrete digestive enzymes that liquefy dead tissue, which they then ingest.
- Their secretions have antimicrobial properties that help reduce the wound's bacterial load.
- Their subtle movements on the wound bed can help stimulate the growth of new, healthy granulation tissue.
This method is remarkably effective for stubborn, non-healing wounds or those infected with antibiotic-resistant bacteria like MRSA. While it takes some getting used to for patients, it's a highly effective, painless, and well-established medical procedure.
Comparison of Wound Debridement Techniques
Choosing the right debridement method is a clinical decision based on a careful assessment of the wound, the patient, and the treatment goals. Each technique has its own profile of benefits and drawbacks.
The table below offers a quick, side-by-side comparison to help illustrate where each method shines.
| Technique | Selectivity | Speed | Pain Level | Ideal For |
|---|---|---|---|---|
| Surgical/Sharp | High (in skilled hands) | Very Fast | High (requires anesthesia) | Large wounds, advancing infection, urgent cases. |
| Enzymatic | High | Slow | Low / None | Non-surgical candidates, long-term care settings. |
| Autolytic | Very High | Very Slow | None | Stable wounds with minimal debris, palliative care. |
| Mechanical | Low / Non-selective | Moderate | Moderate to High | Wounds with large amounts of loose debris. |
| Biological | Very High | Moderate | Low (mild tingling) | Non-healing wounds, antibiotic-resistant infections. |
As you can see, there's a clear trade-off between factors like speed and selectivity. The fastest method, surgical debridement, requires immense skill and anesthesia, while the most selective and painless method, autolytic debridement, is also the slowest. Ultimately, a skilled wound care professional will often use a combination of these techniques over the life of a wound to achieve the best possible outcome.
How to Select the Right Debridement Technique
Choosing a debridement technique isn't about finding the single "best" method. It’s about picking the right one for the patient in front of you. Think of it like a master chef selecting the right knife: a heavy cleaver is perfect for tough jobs but useless for delicate garnishes.
In the same way, the right debridement method has to perfectly balance the wound's needs, the patient's overall condition, and the resources you have on hand. This is a careful clinical calculation, moving beyond just spotting dead tissue to seeing the whole picture. A successful outcome hinges on matching the technique to the specific goals for that patient at that exact moment in their healing journey.
The Three Pillars of Debridement Decisions
Every solid debridement choice rests on three pillars: the wound, the patient, and the clinical setting. Each one brings up a series of questions that steer you toward the safest, most effective option. If you neglect any one of these pillars, you risk a poor outcome or even creating new complications.
This systematic approach is what turns theory into confident, evidence-based action at the bedside. It provides a clear framework for making the best possible decision.
The flowchart below gives you a simplified decision tree, showing how a factor as basic as urgency can point you toward one technique over another.
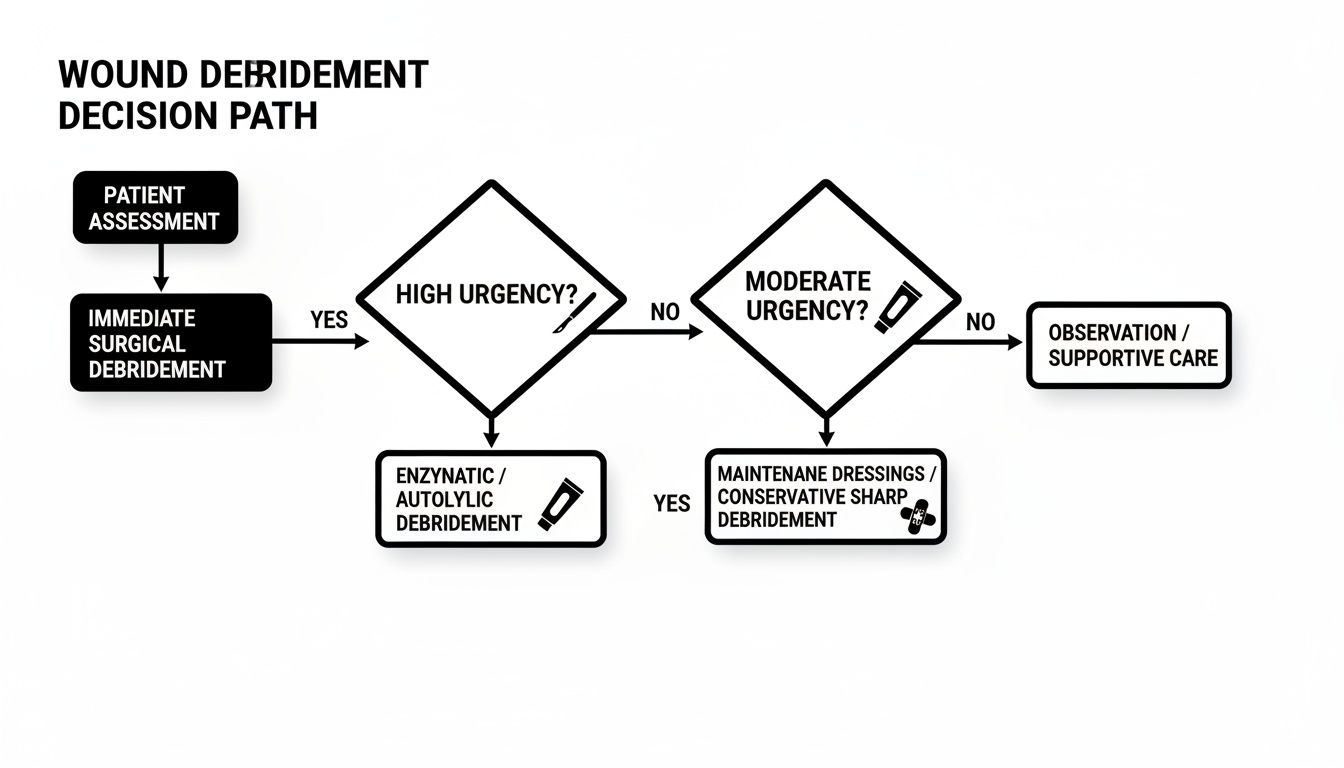
As you can see, high-urgency situations—like a rapidly spreading infection—demand decisive action like sharp debridement. Lower-urgency cases give you the flexibility to use slower, more passive methods.
Assessing the Wound Itself
The wound’s own characteristics are your first and most crucial clue. The type, amount, and location of non-viable tissue will immediately narrow down your choices.
- Urgency and Tissue Type: Are you dealing with thick, leathery eschar or signs of an advancing infection? If so, urgent sharp or surgical debridement is almost always the right call to get that threat under control, fast.
- Infection Status: A clinically infected wound demands a rapid takedown of the bacterial load. Slower methods, like autolytic debridement, simply won't be aggressive enough to win that fight. Advanced tools can help you confirm your suspicions; for example, a point-of-care wound imaging device detects bacterial presence and can guide a more precise debridement strategy.
- Wound Location: Debriding a wound near a major blood vessel, tendon, or prosthetic joint requires extreme precision. In these cases, highly selective and controlled methods like biological or enzymatic debridement might be the safer path.
Here’s a critical rule of thumb: before you debride any wound on a lower extremity, you must assess the vascular supply. Debriding an ischemic wound without adequate blood flow can make healing impossible, potentially creating a larger, more complex wound or even leading to amputation.
Considering the Patient and Their Environment
The patient is always more than just their wound. Their overall health, pain tolerance, and where they are receiving care play a massive role in choosing a debridement strategy that will actually work. A theoretically perfect plan is useless if the patient can't tolerate it or if it's not feasible in their environment.
For instance, a patient with a very low pain threshold or who is taking anticoagulant medication is likely not a good candidate for sharp debridement at the bedside. In that scenario, a gentler approach like enzymatic or autolytic debridement makes far more sense, trading speed for comfort and safety.
Ask yourself these key patient-centered questions:
- Pain Tolerance: Can the patient handle a potentially painful procedure? If not, painless options like autolytic or biological debridement are the way to go.
- Comorbidities: Does the patient have other health issues, like poor circulation or a compromised immune system, that could complicate healing or increase risk?
- Care Setting: Is the patient at home, in a long-term care facility, or in a hospital? The available resources, the skill level of the clinicians, and the frequency of visits all dictate what is practical.
We know these techniques work. In major markets like the US and Europe, where chronic wounds affect 2% of the population (that's 6.5 million Americans every year), debridement has been shown to cut healing times by 20-50%. This is especially true when paired with the moist wound environments that revolutionized care back in the 1960s.
Pairing Debridement with Advanced Wound Therapies
Think of debridement not as the final step in healing, but as the critical opening act. It’s like preparing a garden plot before you plant anything valuable. You have to till the soil, pull the weeds, and clear out the rocks. Only then can you expect the seeds to take root and flourish.
In the same way, advanced wound therapies need a clean, viable wound bed to do their job. Debridement is the process that creates this ideal environment, essentially hitting the reset button on a chronic, stalled wound and making it biologically ready to heal. This partnership between clearing out the old and bringing in the new is the cornerstone of modern wound management.
Guiding Debridement with Diagnostic Tools
Precision is everything. We’ve moved past the days of relying solely on what the naked eye can see. Today’s diagnostic tools give us a detailed map of the wound environment, allowing for a much more targeted and effective approach to debridement.
Take fluorescence imaging, for example. These handheld devices use specific light wavelengths that make certain bacteria glow in real-time. By seeing the exact location and spread of high bacterial loads, we can perform sharp debridement with incredible accuracy, removing only the contaminated tissue while preserving healthy areas. It turns a subjective guess into an objective, guided procedure.
By integrating advanced diagnostics, clinicians can ensure their debridement efforts are focused precisely where they are needed most, maximizing the benefit of each intervention while minimizing trauma to the healing wound bed.
Preparing the Wound Bed for Advanced Therapies
Once the wound bed is properly debrided, it’s primed and ready for a range of powerful, advanced treatments. These therapies are potent, but they all depend on that clean slate to work their magic.
Some of the most common pairings include:
- Negative Pressure Wound Therapy (NPWT): This therapy uses a vacuum to pull fluid from the wound and ramp up blood flow. It’s most effective on a clean wound bed, as any eschar or thick slough would just clog the system and block the benefits.
- Cellular and Tissue-Based Products (CTPs): Think of these as advanced biological dressings, like skin substitutes or amniotic allografts, that introduce new cells and growth factors to jumpstart regeneration. Applying them to a non-debrided wound is like trying to plant seeds on concrete—the valuable cells have nowhere to go and nothing to integrate with.
- Hyperbaric Oxygen Therapy (HBOT): This treatment floods the body with pure oxygen in a pressurized room to accelerate healing. Its effectiveness is multiplied when that oxygen-rich blood can get to a clean, well-vascularized wound bed that’s been cleared by debridement.
This focus on evidence-based practice marks a huge shift from older methods. A key breakthrough in the 1960s showed that moist wounds healed 50% faster than dry ones, which changed everything and led to the occlusive dressings we rely on today. Now, with over 5,000 products available—from alginates that can absorb 20 times their weight to bioengineered skins—proper wound bed preparation is more critical than ever.
When we use these advanced therapies, it’s vital to track their performance, which underscores the importance of outcome measurement in clinical practice. A well-debrided wound also creates the perfect surface for a dual-layer allograft to adhere properly and support tissue growth, bridging the gap between a clean wound and complete closure.
Common Questions About Wound Debridement
Even when you understand the different debridement techniques, it's natural to have practical questions about what to expect. Answering these common concerns is a huge part of managing expectations, keeping patients comfortable, and showing just how vital this step is for healing.
Let's walk through some of the questions we hear most often from both patients and clinicians.
Is Wound Debridement a Painful Procedure?
The honest answer? It depends entirely on the method we use.
Surgical or sharp debridement can definitely be painful, which is exactly why we always use local or topical anesthetics to make sure the patient is comfortable. Mechanical debridement can also cause some pain, especially when old dressings are removed from the wound bed.
On the other hand, autolytic and enzymatic debridement are usually painless because they work so slowly and selectively. Larval therapy might cause a mild tingling sensation, but that’s typically it. A good clinician will always talk through pain management options beforehand to make the whole process as comfortable as possible.
How Often Does a Wound Need Debridement?
The frequency really comes down to the wound's condition and the technique we've chosen. For a wound with a lot of necrotic tissue, we might start with an aggressive sharp debridement and then schedule regular follow-ups, often weekly, to keep it clean.
Many chronic wounds need what we call "maintenance debridement" to stop non-viable tissue and biofilm from building back up. With slower methods like autolytic debridement, the process is actually continuous with every single dressing change. We’ll assess the wound bed at every visit to decide if more debridement is needed to keep the healing on track.
A key takeaway is that debridement is not always a one-time event. For many chronic wounds, it becomes a recurring part of the care plan to keep the wound bed clean and progressing toward closure.
Can Debridement Make a Wound Worse?
When a trained professional performs debridement correctly, the benefits to healing are overwhelming. But like any medical procedure, there are some risks. If non-selective methods are used improperly, they can damage healthy granulation tissue and actually slow things down.
It's also absolutely critical to check a patient's vascular supply before performing sharp debridement on an ischemic limb, as this could accidentally create a much larger wound. A thorough assessment of both the patient and the wound is non-negotiable—it’s how we pick the right method and ensure the benefits far outweigh any potential risks. The goal is always to remove barriers, not create new ones.
The field is constantly improving, with newer approaches making traditional methods even better. For instance, Negative Pressure Wound Therapy (NPWT) can speed up debridement by 30-40%, while hyperbaric oxygen therapy helps 85% of wounds that just won't heal. Even ancient practices like larval therapy are making a comeback, clearing stubborn biofilms in just 72 hours and cutting treatment costs by 25%. You can read more about the evolution of wound care practices to see how far we've come.
At Specialty Wound Care, we pair precise debridement with the most advanced diagnostic and therapeutic tools available. Our goal is to create an optimal healing environment for every patient, reducing healing times and helping you return to your life. Learn more about our comprehensive approach to managing complex wounds.