To really get a handle on venous leg ulcer treatment, you have to start with the root cause: veins that aren't working right. Think of it as a plumbing problem in your legs. When blood flow stalls, pressure builds up and starts damaging the skin from the inside out. To heal the wound, we have to tackle that pressure head-on and create the perfect environment for the skin to mend itself.
What Causes Venous Leg Ulcers to Form
Before you can fix a venous leg ulcer, you have to understand why it showed up in the first place. Imagine the veins in your legs are a one-way street, designed to push blood back up to your heart against gravity. This street is lined with tiny gates—or valves—that snap shut to stop blood from flowing backward.
But what happens when those gates get weak or fail? Blood starts to pool in your lower legs, creating a constant traffic jam. This condition is called chronic venous insufficiency, and it causes a slow, relentless rise in pressure inside the veins, a state we call venous hypertension.
From Hidden Pressure to Open Wound
This constant pressure is like a slow-motion flood inside your leg. Fluid, proteins, and even blood cells begin to leak out of the overwhelmed veins and into the surrounding tissue. This process essentially starves the skin of the oxygen and nutrients it needs to stay healthy. It becomes fragile, discolored, and swollen.
After a while, the skin gets so compromised that even a tiny bump, a simple scratch, or an insect bite can be enough to break it open, forming an ulcer. And because the underlying circulation problem is still there, the wound can't get the resources it needs to heal. That's what makes these ulcers so notoriously stubborn.
Venous ulcers are the most common type of chronic wound on the lower legs, affecting millions of adults. They aren't just a skin issue; they are a direct signal of an underlying vein disease that requires specialized medical attention to fix for good.
The Growing Need for Effective Treatment
This is a massive public health challenge. The global market for treating venous leg ulcers was valued at USD 2.96 billion back in 2018, and it's projected to climb to USD 7.21 billion by 2032. This isn't just a number; it reflects the real-world increase in chronic venous insufficiency, especially as our population ages.
The toll these wounds take, both financially and personally, highlights just how critical it is to get prompt, expert care. You can't just slap a bandage on the problem and hope for the best. Addressing the vein issues underneath is non-negotiable if you want lasting recovery and to stop the ulcer from coming back.
Visiting dedicated vein health clinics is a crucial first step. It's the only way to break the frustrating cycle of a wound that just won't heal. By tackling the root cause, we can finally move past just "managing" the wound and start achieving complete, durable healing.
Why Compression Therapy Is the Gold Standard Treatment
To actually heal a venous leg ulcer, you have to treat the root cause—not just put a bandage on the wound. This is where compression therapy comes in, and it's the undisputed gold standard for a reason. It works by applying steady, external pressure to the leg, directly fighting back against the damaging effects of venous hypertension.
Think of it this way: the veins in the leg have become weak, like a stretched-out rubber band. They can't effectively snap back to push blood up toward the heart. Compression bandages or wraps act as an external support system, giving the leg a gentle squeeze that helps those veins get their job done.
This simple mechanical support is powerful. It pushes pooled blood and excess fluid out of the lower leg and back into circulation. As a result, swelling goes down, more oxygen reaches the skin, and the wound finally has the right environment to start healing. Trying to heal a VLU without compression is like trying to bail out a boat with a hole in it—you're just fighting a losing battle against the underlying problem.
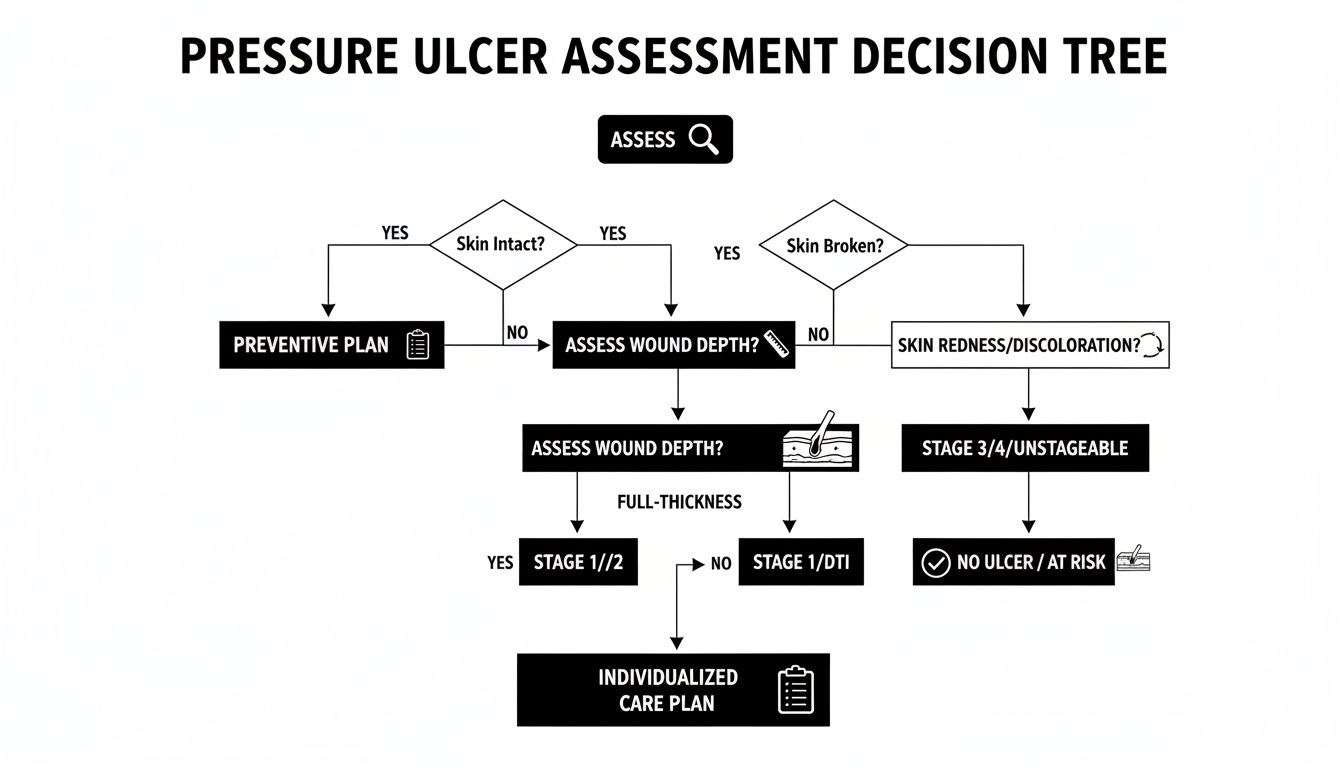
The diagram below shows exactly how venous insufficiency kicks off the chain reaction that compression is designed to stop.
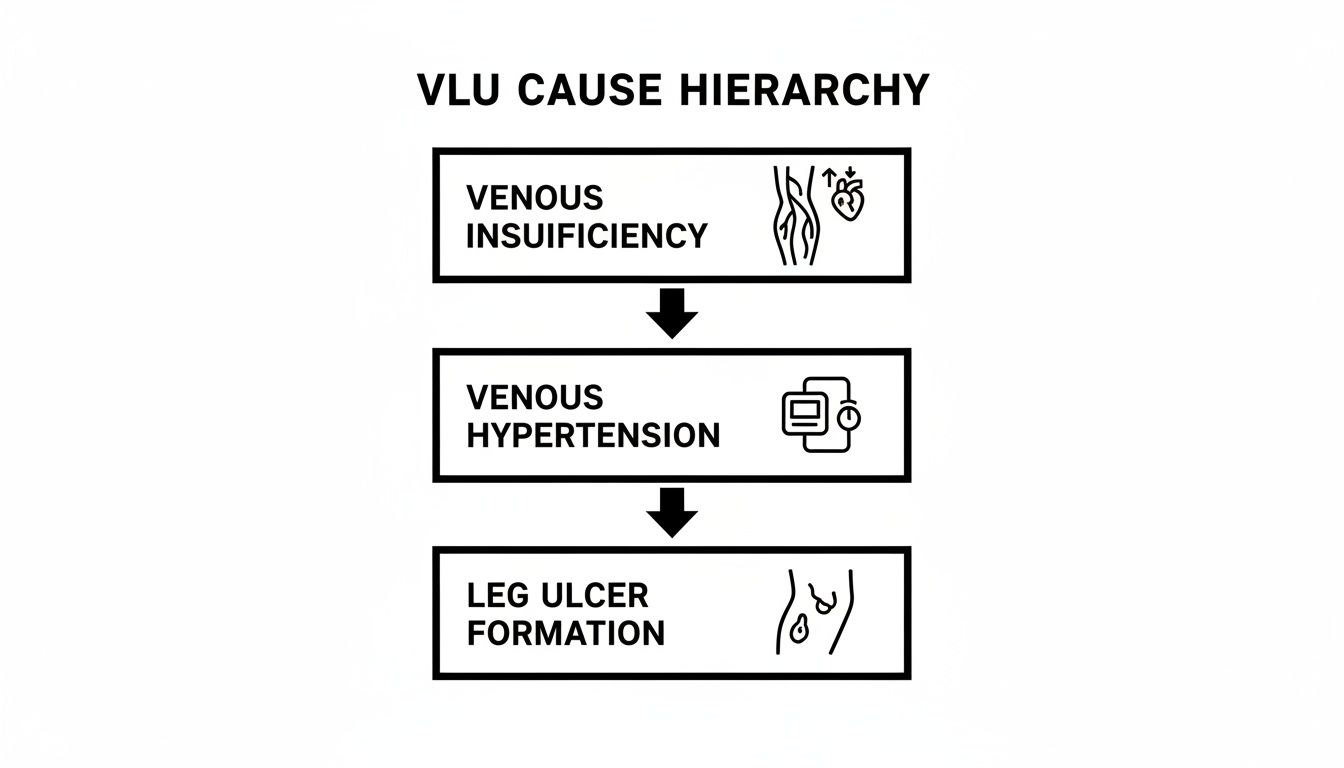
As you can see, the ulcer is just the final, visible symptom of a deep-seated circulatory failure. That’s why applying external pressure is a non-negotiable part of the solution.
Choosing the Right Compression System
Not all compression is created equal. The right system depends entirely on the patient's situation, the condition of the wound, and who will be applying it. There are several go-to options, and each has its own strengths.
Common compression systems include:
- Multi-Layer Compression Bandages: These are often the first choice when starting treatment. Made up of several layers, they provide high, sustained pressure and have to be applied by a trained clinician. They typically stay on for several days at a time.
- Adjustable Compression Wraps: These systems use Velcro straps, which makes them much easier for patients or their caregivers to put on and adjust. They strike a great balance between effective compression and ease of use, which can make all the difference for long-term compliance.
- Compression Stockings: While they are absolutely essential for preventing another ulcer after the current one has healed, stockings are notoriously difficult to pull on over an open wound. They come in different pressure levels and are key to stopping the cycle of recurrence.
Deciding which system to use is a clinical judgment call that should only be made after a complete assessment of the patient's leg, the ulcer, and their overall health.
Before diving deeper, this table breaks down the key differences between the most common compression therapy options, helping clarify which might be best for different clinical scenarios.
Comparing Compression Therapy Systems
| System Type | Key Features | Ideal For | Application Frequency |
|---|---|---|---|
| Multi-Layer Bandages | Provides sustained, high, non-removable pressure. Requires professional application. | Initial treatment of active VLUs, especially with significant edema. Patients who may not be compliant with removable systems. | Every 3-7 days |
| Adjustable Wraps | Velcro-based systems that are user-friendly. Allows for self-application and adjustment. | Patients needing a balance of high compression and ease of use. Good for transitioning from multi-layer systems. | Daily (applied by patient/caregiver) |
| Compression Stockings | Prescribed pressure garments worn daily. Can be difficult to apply over an open wound. | Long-term prevention after the ulcer has healed. Maintaining circulatory health. | Daily |
| Two-Layer Systems | A simpler alternative to 4-layer systems, often combining a padded layer and a cohesive compression layer. | Patients who find 4-layer systems too bulky or for managing less severe edema. | Every 3-7 days |
Understanding these distinctions is the first step in tailoring a compression plan that a patient can actually stick with, which is the key to success.
The Critical Role of Consistent Application
The best compression system in the world is useless if it isn't used correctly and consistently. Sporadic use just won't cut it. The pressure has to be applied the right way—every single day—to keep venous hypertension in check and give the wound a fighting chance.
The success of compression therapy is not just in the product itself, but in the faithful, day-in-day-out application. It is the single most important factor in promoting healing and preventing the ulcer from returning.
This commitment can be a huge challenge for patients, but it’s the foundation that all other treatments are built on. The numbers back this up: compression therapy dominates the VLU market, accounting for 40% of spending, because it's the only way to counteract the underlying cause.
Studies have shown that consistent compression can slash healing time by 30-50%. It’s also the best defense against recurrence, which can happen in up to 40% of patients within a year if they stop therapy. You can find more data on the venous leg ulcer market on Precedence Research.
Ultimately, proper application ensures the pressure is graduated—tightest at the ankle and gradually decreasing up the leg—to give blood flow the upward push it needs. This consistent, correctly applied pressure is what makes compression therapy the true cornerstone of VLU healing.
How to Prepare the Wound Bed for Healing

While compression gets to the root of the circulatory problem, we can't just ignore the wound itself. Think of preparing a wound bed like tending a garden. Before you can expect new seeds to sprout, you have to clear out all the weeds, rocks, and dead leaves.
In wound care, this essential "weeding" is called debridement. A venous leg ulcer is often covered in non-viable tissue—like yellowish slough or black eschar—that physically blocks new cells from growing. Even worse, this dead tissue is a five-star hotel for bacteria, inviting infection and bringing the healing process to a dead stop.
The Importance of Debridement
Debridement is the absolute cornerstone of local wound care. It’s the process of carefully removing all that unhealthy tissue to expose the healthy, bleeding wound bed underneath. This is the "fertile soil" where new granulation tissue can finally start to grow. Skipping debridement is like trying to build a house on a crumbling foundation; it’s just not going to work.
There are several ways to get the job done, and the right method depends on the situation:
- Sharp Debridement: A clinician uses a scalpel or special scissors to precisely cut away the dead tissue. This is often the fastest way to remove a large amount of unhealthy material.
- Enzymatic Debridement: A prescription ointment with special enzymes is applied directly to the wound. Over time, these enzymes work to chemically dissolve the dead tissue.
- Autolytic Debridement: This is the most natural approach, using the body's own enzymes to break down non-viable tissue. We encourage this process by keeping the wound moist with specific dressings.
The best choice depends on how much dead tissue there is, the patient’s overall condition, and the clinician's expertise. A skilled provider knows exactly which tool to use to get the wound bed ready for healing.
Cleansing and Maintaining Moisture Balance
Once the weeds are gone, the garden needs just the right amount of water—not a flood, and not a drought. The same exact principle applies to a wound bed. You need proper cleansing and the perfect moisture balance for a VLU to heal.
Cleansing usually involves gently flushing the wound with a non-toxic solution, like sterile saline, to wash away loose debris and lower the bacterial count. Aggressive scrubbing is a big no-no, as it can easily damage the fragile new cells we’re trying to encourage.
Maintaining a moist wound environment is a fundamental concept in modern wound care. A wound that’s too dry will kill off new cells, but a wound that’s too wet can damage the healthy skin around it. The goal is that perfect equilibrium.
We use specialized dressings to manage the wound's moisture level. If a wound has heavy drainage, we'll choose an absorbent dressing to pull the excess fluid away. For a drier wound, we’ll use a dressing that donates moisture back to it. This careful management creates the ideal environment for cells to migrate across the wound bed and finally close the gap.
For those especially stubborn wounds, advanced treatments like a dual-layer allograft can provide a scaffold to support cell migration and kickstart healing. By combining debridement, cleansing, and moisture balance, we give the body its best possible shot at rebuilding and recovering.
Advanced Therapies for Non-Healing Ulcers
Sometimes, even with perfect compression and diligent wound care, a venous leg ulcer just refuses to heal. These stubborn, non-healing wounds can be incredibly frustrating for both patients and clinicians. When a wound stalls, it’s a clear sign it needs more than basic support; it requires a more advanced intervention to get the healing process back on track.
This is where the next level of venous leg ulcer treatment comes into play. These therapies are designed to give the body a powerful boost, tackling the biological roadblocks that keep a wound stuck in a chronic, inflammatory state. They move beyond just managing the environment and actively stimulate the body’s own regenerative capabilities.

Bioengineered Skin Substitutes
Imagine trying to build a new wall where the old one crumbled, but you have no framework to guide you. That’s the challenge the body’s cells face when trying to close a chronic wound. Bioengineered skin substitutes, also known as cellular and tissue-based products (CTPs), provide that missing framework.
These products act as a biological scaffold. Applied directly to the prepared wound bed, they deliver essential components like collagen, growth factors, and sometimes even living cells. This scaffold gives the body's own skin cells a structure to crawl across, encouraging them to migrate, multiply, and rebuild lost tissue much faster than they could on their own.
There are many types of skin substitutes available, each with its own unique properties:
- Allografts: Sourced from human donor tissue (like amniotic membrane), these provide a rich matrix of growth factors that signal the body to calm inflammation and start rebuilding.
- Xenografts: Derived from animal sources, these primarily offer a collagen scaffold that supports new tissue formation.
- Synthetic Options: Lab-created materials designed to mimic the skin's natural structure, providing a clean and consistent framework for cellular growth.
The choice of product depends on the specific needs of the wound, but the goal is always the same: to jumpstart a healing process that has come to a grinding halt.
Negative Pressure Wound Therapy
Another powerful tool for these non-healing ulcers is Negative Pressure Wound Therapy (NPWT). This involves placing a specialized foam dressing over the wound, sealing it with a clear film, and connecting it to a small vacuum pump. The pump then creates a gentle, continuous negative pressure—or suction—over the entire wound bed.
Think of NPWT as a system that does two critical jobs at once. First, it actively pulls excess fluid and infectious material away from the wound, keeping it clean and dramatically reducing swelling. Second, this gentle suction stimulates blood flow to the area, drawing in the oxygen and nutrient-rich blood that’s vital for fueling new cell growth.
NPWT transforms a passive wound environment into an active one. By physically contracting the wound edges and promoting the formation of healthy granulation tissue, it can significantly accelerate healing in complex cases that have failed to respond to other treatments.
This technology has become a go-to solution for deep, heavily draining, or otherwise complicated wounds that need intensive management to get them ready for closure.
Uncovering Hidden Bacteria with Fluorescence Imaging
One of the biggest enemies of wound healing is bacteria, especially when it forms a hidden, slimy layer called biofilm. Traditional swabs can easily miss these entrenched bacterial colonies, leaving clinicians guessing why a wound isn't progressing. Fluorescence imaging is a game-changing diagnostic tool that finally makes the invisible visible.
This handheld device shines a safe, violet light onto the wound. In response, different tissues and bacteria glow in specific colors. Healthy tissue might glow green, while harmful bacteria like Pseudomonas aeruginosa light up in a distinct red or cyan.
This real-time bacterial map allows clinicians to:
- Pinpoint Contamination: See exactly where high bacterial loads are hiding, even if they aren't visible to the naked eye.
- Guide Debridement: More accurately remove contaminated tissue while preserving healthy areas.
- Improve Sampling: Take cultures from the most problematic spots to get accurate diagnostic results.
By revealing the true bacterial burden of a wound, fluorescence imaging enables a much more targeted and effective venous leg ulcer treatment plan. This approach is part of a growing trend toward using advanced tools to solve complex healing challenges. The market for these technologies reached USD 2.1 billion in 2023 and is projected to hit USD 3.3 billion by 2034, driven by the proven success of NPWT and bioengineered dressings. You can discover more insights about the venous leg ulcer market on Biospace.
When standard protocols are not enough, these advanced options provide new hope. You can learn more about how these therapies are integrated into a complete care plan by exploring our guide on advanced treatment options by Primus Specialty Wound Care.
Building a Long-Term Plan to Prevent Recurrence
Getting a venous leg ulcer to finally heal is a huge accomplishment, but it's really only half the battle. The root cause of the ulcer—that pesky condition called chronic venous insufficiency—doesn't magically go away once the skin closes. This means without a solid long-term plan, the odds of that ulcer coming back are incredibly high.
Think of it like patching a leak in your roof. You can fix the spot that’s dripping, but if you don’t address the damaged shingles, the next big storm will have water pouring right back in. Preventing another ulcer requires a mental shift from treating a wound to managing a lifelong condition.
The best long-term strategy puts you in the driver's seat. It's all about building a consistent daily routine that supports your vein health and protects your skin. It’s the only way to break the painful cycle for good.
The Lifelong Commitment to Compression
Let's be clear: the single most important part of any prevention plan is lifelong compression therapy. The very same tool that helped heal your ulcer is the one that will stop a new one from ever starting. Wearing your prescribed compression stockings or wraps every single day is completely non-negotiable.
Compression garments do the heavy lifting that your veins can't. They give your legs the external support needed to keep blood from pooling and venous pressure from rising. Skipping even a day or two can be enough to let fluid build up, putting your fragile, newly-healed skin at risk all over again.
Without ongoing care like consistent compression and regular skin checks, venous leg ulcers have a high rate of recurrence. Lifelong management is the key to preventing this frustrating and painful cycle from repeating.
Your doctor will help you find the right type of garment and the correct pressure level for long-term wear. It might feel like a chore at first, but making compression part of your daily routine—just like brushing your teeth—is the strongest defense you have.
Empowering Yourself with Daily Habits
Beyond compression, a few simple but powerful lifestyle habits can make a massive difference in preventing another VLU. When done together, these habits work to ease the strain on your veins and keep your skin tough and resilient.
A strong prevention plan should include:
-
Leg Elevation: Any time you're sitting down for a while, prop your legs up so your feet are higher than your heart. This simple trick uses gravity to your advantage, helping drain pooled blood from your lower legs and giving your veins a much-needed break. Try to do this for 30 minutes, three or four times a day.
-
Appropriate Exercise: Movement is medicine for your veins. Your calf muscle acts like a powerful pump, squeezing the veins and pushing blood back toward your heart every time you take a step. Low-impact activities like walking are perfect for getting this "calf muscle pump" working.
-
Daily Skin Care and Inspection: The skin on your lower legs will always be a bit more fragile after an ulcer. Keep it strong by moisturizing every day with a pH-balanced, fragrance-free lotion to prevent dryness and cracking. Just as important, give your legs and feet a quick look-over every single day. Watch for any signs of trouble like redness, new discoloration, or tiny breaks in the skin. Catching a problem when it's small is everything.
Building Your Long-Term Care Team
You don't have to manage this alone. Think of it as a team effort, and you're the star player. But every star player needs a good coach, and that means having specialists in your corner. Regular follow-up appointments with a vein specialist or wound care clinic are vital, even when you feel perfectly fine.
These check-ups are where your provider can:
- Check your circulation, often with a quick ultrasound.
- Make sure your compression garments still fit right and are providing enough pressure.
- Spot any early skin changes before they have a chance to turn into a new wound.
Staying in touch with your care team keeps your prevention plan sharp and effective. By combining daily compression, healthy habits, and ongoing professional guidance, you can slash the risk of recurrence and take back control of your long-term leg health.
Common Questions About Venous Leg Ulcer Treatment
When you're dealing with a venous leg ulcer, a lot of questions pop up. Getting clear, honest answers is the first step toward feeling in control of your health. Let’s tackle some of the most common concerns to clear things up and give you the confidence you need for a successful recovery.
Knowing what to expect—and what to watch out for—can make all the difference in your healing journey.
How Long Does a Venous Leg Ulcer Typically Take to Heal?
This is usually the first question on everyone's mind, and the most truthful answer is: it really depends. There’s no magic number. The healing timeline is shaped by a few key things: the ulcer's size and depth, how long it's been there, your overall health, and—most critically—how closely you stick to your treatment plan.
With consistent, top-notch care that includes proper compression therapy and wound management, smaller ulcers can heal up in about 3 to 4 months. For larger, deeper, or more stubborn ulcers that have been around for a while, the process can easily take 6 to 12 months, sometimes even longer.
The single most important factor in speeding up healing is sticking to the plan your specialist creates. It’s the daily consistency with compression, wound care, and lifestyle adjustments that separates a wound that heals from one that just won't go away.
Patience and persistence are your best friends here. You have to remember, we're not just healing skin; we're fixing the underlying circulation problem that caused the ulcer in the first place.
Can I Treat a Venous Leg Ulcer Myself at Home?
While what you do at home is absolutely essential, a venous leg ulcer is not something you should ever try to manage on your own. This condition demands professional medical supervision from beginning to end. A wound care specialist needs to accurately diagnose the issue and make sure other serious problems, like arterial disease, aren't being missed.
Think of it like a partnership. Your healthcare provider is the coach, and you're the star player.
The provider's job is to:
- Get the Diagnosis Right: Using tools like ultrasound to confirm it's actually venous insufficiency.
- Prescribe the Right Compression: Figuring out the exact level of pressure your leg needs.
- Perform Debridement: Safely cleaning the wound by removing dead tissue so healthy cells can take over.
- Watch for Infection: Catching and treating bacterial issues before they become a major problem.
Your role at home is to follow the playbook they design for you. That means wearing your compression gear faithfully, elevating your leg, moving around, and never skipping an appointment. Trying to go it alone can lead to serious trouble, including out-of-control infections, a wound that gets worse, and a much, much longer healing time.
What Are the Signs My Ulcer Is Infected or Getting Worse?
Knowing the red flags for infection is one of your most important jobs in managing your wound at home. An infection that goes untreated can completely derail the healing process and lead to bigger health issues. You need to call your healthcare provider right away if you notice any of these changes.
Key Warning Signs of Infection:
- More Pain: A sudden spike in pain or a new type of pain around the wound that feels different from the usual discomfort.
- Spreading Redness: The skin around the wound becomes red and warm, and that redness starts creeping outward.
- A Bad Smell: A distinct, foul odor coming from the wound, even right after it's been cleaned.
- Changes in Drainage: The amount of fluid coming from the wound suddenly increases, or it changes color to a cloudy, yellow, or green.
- Feeling Sick: You start running a fever, get the chills, or just feel generally unwell. This could mean the infection is spreading through your body.
Catching an infection early is everything. Don't ever hesitate to call your doctor or wound clinic if you even think something is wrong. It's always better to be safe and get a professional opinion than to wait and let a small issue turn into a huge setback for your venous leg ulcer treatment. Early action usually means a quick course of antibiotics and getting your healing journey right back on track.
At Specialty Wound Care, we combine advanced diagnostics with expert clinical care to create personalized treatment plans that accelerate healing. If you or a loved one is struggling with a non-healing wound, our team is here to help. Discover how our evidence-based approach can make a difference by visiting us at https://specialtywoundcare.com.