Preventing a surgical site infection isn’t a single action, but a coordinated effort that spans the entire surgical journey—before, during, and after your procedure. It's a partnership between you and your care team. Success hinges on optimizing your health beforehand, ensuring absolute sterility in the operating room, and staying vigilant with wound care during recovery.
Honestly, the most effective strategy is simply to follow your care team's guidance at every single step.
Why We Have to Talk About Surgical Site Infections
A surgical site infection (SSI) is so much more than a clinical term. For a patient, it’s a major setback on the road to recovery. It’s what happens when germs find their way into a surgical incision, triggering complications that can be as minor as a little redness or as severe as a life-threatening condition.
When an infection takes hold, it almost always means a longer, more painful recovery. It means more trips to the doctor, more antibiotics, and sometimes, another operation to fix the problem. The emotional and financial toll on patients and their families is immense.
Just How Big is the Problem?
Surgical site infections are a stubborn, global healthcare challenge. They are consistently one of the most common—and frustratingly, preventable—complications after surgery.
Globally, SSIs affect 2% to 4% of all patients who have an inpatient procedure. Here in the United States, that translates to over 400,000 extra hospital days every year, with a staggering price tag of around $900 million. Worldwide, the average incidence is about 2.5%, but that number can skyrocket to over 11% in regions with fewer resources. You can dig deeper into these SSI statistics and see the real impact on patient safety.
This isn’t just a numbers game; it’s about patient safety and the quality of care we deliver. To see how these principles fit into the bigger picture, it's helpful to understand the core strategies used to prevent healthcare-associated infections across all medical settings.
Here's the most important thing to remember: a huge number of these infections are completely avoidable. With proven, evidence-based strategies, healthcare teams and patients can work together to bring that risk way down and pave the way for a smoother, safer recovery.
A Roadmap for Prevention
This guide breaks down SSI prevention into three distinct phases. Think of it as a game plan where every stage has clear, actionable steps for both you and your clinical team.
- The Pre-Operative Phase: This is all about getting your body ready for surgery. We'll cover how to optimize your health, what’s involved in proper skin prep, and why the timing of pre-surgical antibiotics is so critical.
- The Intra-Operative Phase: Next, we'll go inside the operating room. We’ll look at the non-negotiables, from maintaining a sterile field to the surgical safety checklists that protect every patient.
- The Post-Operative Phase: Finally, we’ll talk about your role after the procedure. This is where proper wound care, knowing the early warning signs of infection, and understanding when to call for help make all the difference.
Your Pre-Operative Playbook for Infection Defense
Preventing a surgical site infection doesn't start the moment you're wheeled into the OR. The real work begins days, and sometimes weeks, beforehand. Think of this pre-operative phase as setting the stage—getting your body in the best possible shape for a smooth, infection-free recovery.
It all starts with a frank conversation and a thorough risk assessment with your surgeon. This isn't just a box-ticking exercise; it's a critical look at your personal health factors that could put you at a higher risk. Being open about your medical history and lifestyle is absolutely essential here.
This flowchart breaks down the simple, three-phase approach to keeping infections at bay, showing what happens before, during, and after your procedure.
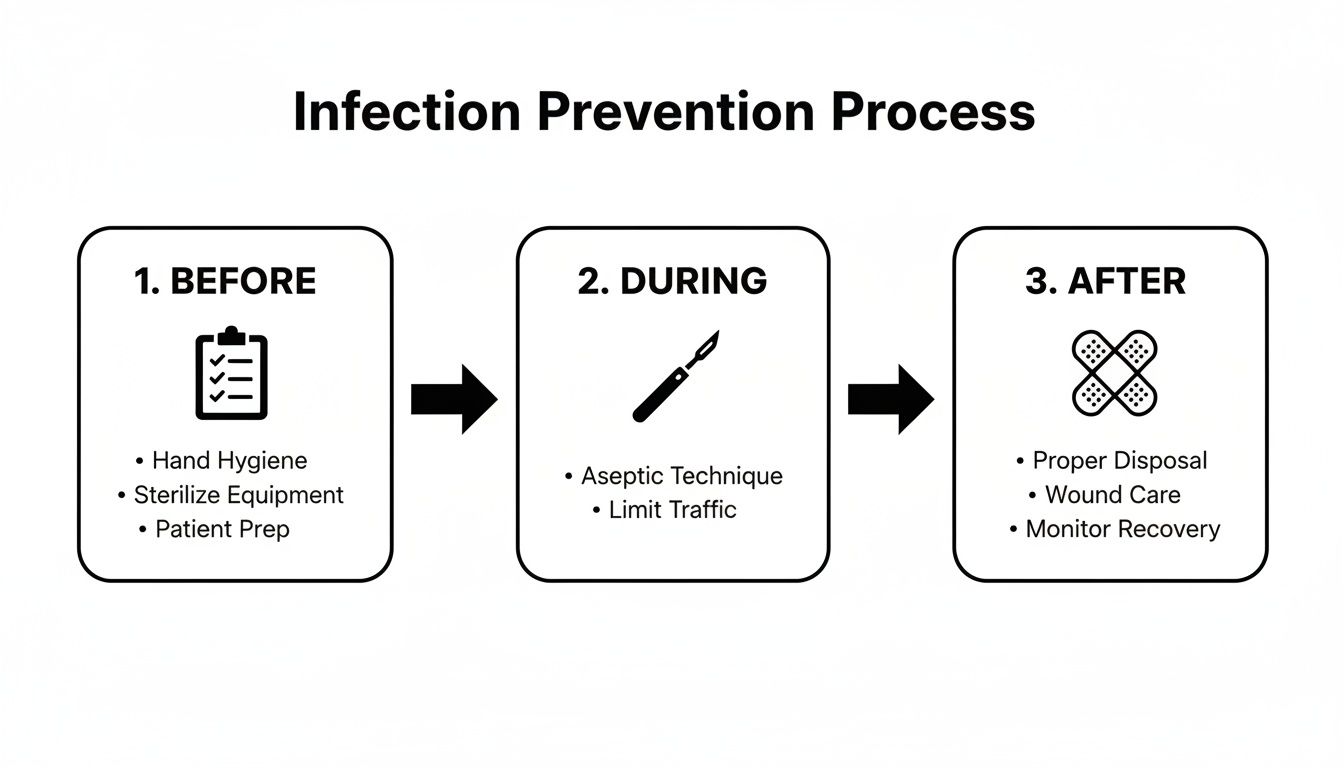
As you can see, infection control is a continuous loop, but optimizing your health before surgery is the foundation everything else is built on.
Getting Your Body Ready for Surgery
Once we know the risks, we can work on them. This is what we call "optimization"—taking proactive steps to manage any health issues that might interfere with your body's natural defenses.
For example, out-of-control blood sugar is a major red flag. High glucose levels can cripple your white blood cells, the very soldiers that fight off bacteria. If you're diabetic, your surgical team will want to see that your blood sugar is stable and well-managed leading up to the big day.
Smoking is another huge one. Nicotine clamps down on your blood vessels, which chokes off the supply of blood and oxygen to the surgical site. Oxygen is non-negotiable for healing tissue and for your immune cells to do their job. The good news? Quitting smoking even four to six weeks before surgery can make a massive difference in your outcome and slash your infection risk.
Skin Preparation and Hair Removal
Your skin is your body's first line of defense, but it's also covered in bacteria. The goal of skin prep is to reduce the number of these microbes at the incision site without causing any new problems.
Years ago, we used to shave the area. We know better now. Razors create tiny nicks and scrapes in the skin—basically, open invitations for bacteria to get in.
Today, the gold standard is simple: we only remove hair if it's absolutely necessary, and we use electric clippers. Clippers trim the hair right at the surface without breaking the skin. It’s a small change in practice that has had a huge impact on preventing surgical site infections.
Your surgeon will likely also send you home with a special antiseptic wash, usually one containing chlorhexidine gluconate (CHG). You'll be instructed to shower with it the night before and the morning of your surgery. It’s a simple task that dramatically lowers the bacterial count on your skin. Follow the instructions to the letter.
- Use the antiseptic soap exactly as directed, focusing on the surgical area.
- Skip the lotions, deodorants, or powders after you wash. They can reduce the soap's effectiveness.
- Sleep on fresh, clean sheets the night before surgery to keep your skin as clean as possible.
The Role of Prophylactic Antibiotics
Even with perfect preparation, some bacteria might still hang around. That's where prophylactic antibiotics come into play. We give you a dose of antibiotics right before your surgery starts to give your body a head start against any potential invaders.
Timing is everything. For the antibiotics to work, they have to be in your bloodstream when the surgeon makes the first incision. The standard is to administer the IV antibiotic within 60 minutes before that first cut.
The choice of drug isn't random, either. Your team selects an antibiotic that is known to be effective against the bacteria most likely to cause an infection for your specific type of surgery. It’s a targeted, preventative shield—not a treatment for an infection you already have. This proactive step is a cornerstone of modern surgical safety.
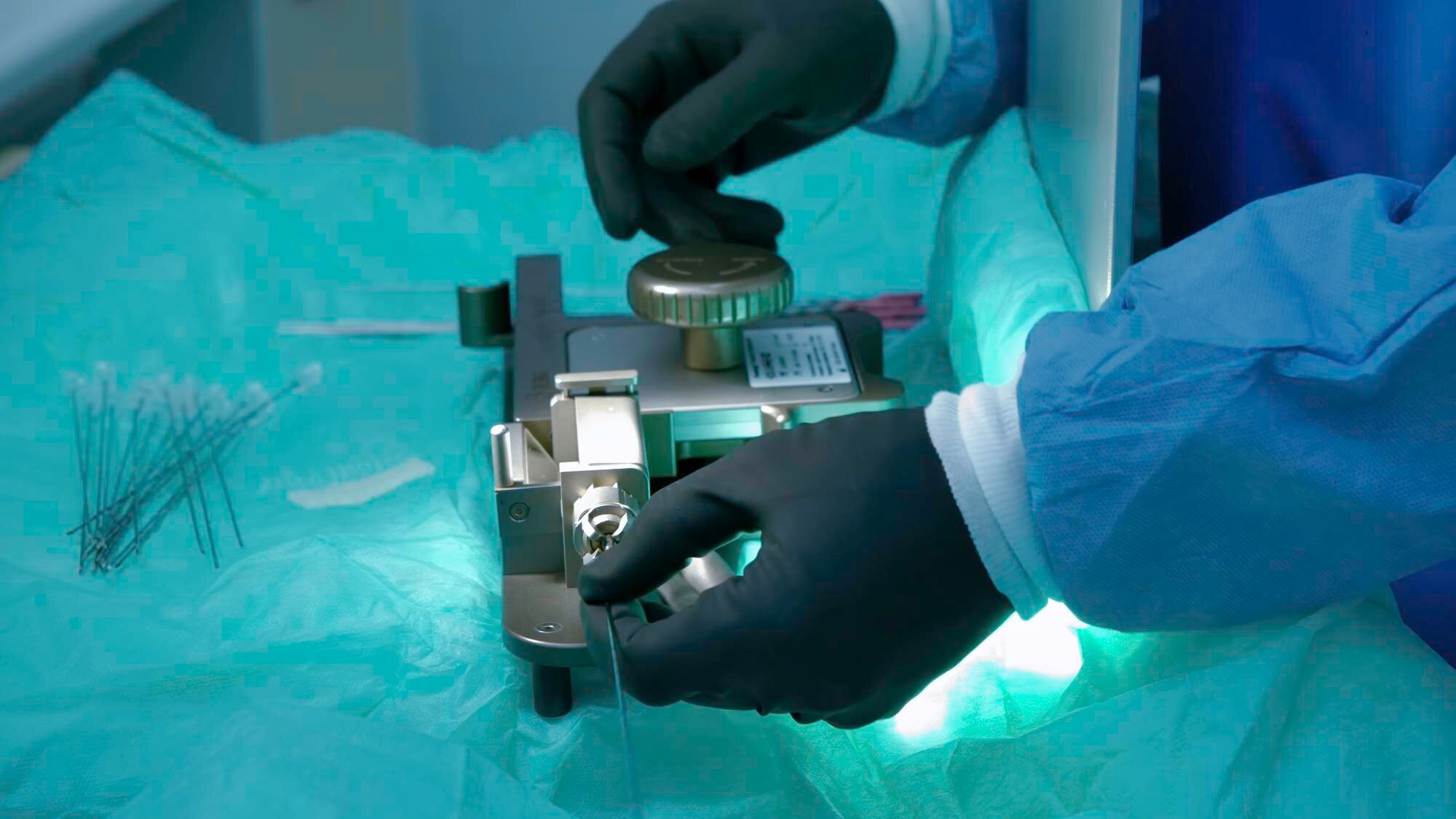
Inside The Operating Room: Proactive Measures During Surgery
Once a patient enters the operating room, the responsibility for preventing infection shifts entirely to the surgical team. This is where a symphony of practiced, evidence-based protocols comes together in a highly controlled environment to ensure patient safety. While you won't be awake to see it, understanding what happens behind the scenes can offer tremendous peace of mind.

The absolute cornerstone of safety inside the OR is aseptic technique. This isn't just about wearing gloves; it's a rigorous, multi-layered approach to minimizing contamination at every turn. It all starts with meticulous hand hygiene, where surgeons and nurses perform a detailed surgical scrub. Just as critical are the essential medical device sterilization methods that guarantee every instrument used is completely free of microorganisms.
From there, the team establishes and strictly maintains a sterile field—a designated area around the patient where only sterile items are permitted. Every drape, tool, and gloved hand entering this zone must meet uncompromising standards. Any breach, no matter how small, demands immediate corrective action to protect the patient.
Beyond The Sterile Field: Controlling The Environment
Preventing surgical site infections also involves controlling the operating room environment itself. These factors are often invisible but play a powerful role in keeping patients safe.
Operating rooms are engineered with specialized ventilation systems that use positive-pressure airflow and high-efficiency particulate air (HEPA) filters. This setup constantly pushes clean, filtered air into the room while forcing potential airborne contaminants out, dramatically reducing the number of microbes in the air.
One of the most significant yet underappreciated strategies is maintaining the patient's core body temperature. When a patient gets cold during surgery (hypothermia), it can weaken their immune response and decrease blood flow to the surgical site. Simply keeping the patient warm—a practice called normothermia—has been shown to reduce SSI risk by as much as three-fold.
To provide a clearer picture, here’s a breakdown of the key interventions that happen while a patient is on the operating table.
Key Intra-Operative Prevention Strategies
This table summarizes the core evidence-based interventions performed during surgery to minimize the risk of surgical site infections.
| Intervention | Rationale and Impact |
|---|---|
| Antimicrobial Prophylaxis | Administering antibiotics within 60 minutes before the first incision ensures peak drug concentration in the tissues, actively fighting bacteria. |
| Aseptic Skin Preparation | Using an alcohol-based chlorhexidine solution has been proven more effective at killing skin flora than older agents like aqueous iodine. |
| Normothermia Maintenance | Keeping the patient's core body temperature stable supports immune function and promotes healthy blood flow and oxygenation to the tissues. |
| Supplemental Oxygen | Providing extra oxygen during and just after surgery can enhance the ability of immune cells to kill bacteria at the surgical site. |
| Gentle Tissue Handling | Minimizing tissue trauma is crucial. Damaged tissue has a weaker defense against infection, so careful surgical technique is paramount. |
These strategies are not just suggestions; they are standard-of-care protocols that form a powerful defense against infection.
Evidence-Based Interventions In Action
Modern surgical care is built on a foundation of proven strategies that actively reduce infection risk. These interventions are often guided by checklists and global health recommendations, ensuring every single patient benefits from the same high standard of care.
Beyond the major points, other practices contribute significantly:
- Efficient Surgery: While never rushing, an experienced surgical team that minimizes the procedure's duration inherently reduces the time the surgical site is exposed to potential contaminants.
- Gentle Tissue Handling: Surgeons are trained to handle tissues with extreme care. Damaged tissue is far more susceptible to infection, making a delicate technique essential.
This entire process is a testament to the detailed planning and execution required for a safe surgical outcome. For those interested in seeing these principles applied, watching professional training videos can offer a deeper appreciation for the skill involved. These coordinated efforts inside the OR create the safest possible environment for your procedure and recovery.
Post-Operative Vigilance: Protecting Your Wound After Surgery
The surgery is over, but your most important job in preventing a surgical site infection is just getting started. The days and weeks that follow are a critical window where your attention to detail can make all the difference. Think of yourself as the most essential member of your own recovery team.

This post-op period is a partnership. Your surgeon has done their part in the operating room; now it’s up to you to follow their instructions to the letter. Doing so protects the delicate healing process and paves the way for a smooth, complication-free recovery.
Mastering Your Wound Care Routine
Those discharge papers aren't just a formality—they're your personalized roadmap to healing safely. At the center of these instructions is proper wound care, and it all starts with one non-negotiable rule: clean hands.
Before you ever touch your dressing or the skin around your incision, wash your hands with soap and water for at least 20 seconds. If that's not possible, an alcohol-based hand sanitizer is your next best option. This simple step is your single most powerful weapon against introducing harmful bacteria to the surgical site.
Your instructions will be very specific about how to handle your dressing. Some of the newer dressings are designed to stay on for several days, while others need to be changed regularly. Don't improvise.
- Follow the Timeline: Change your dressing exactly when you're told to—not sooner, not later.
- Use the Right Supplies: Stick to the sterile gauze and tape provided or recommended by the hospital.
- Keep It Dry: Unless you're explicitly told otherwise, keeping the incision dry is a must. This might mean covering it with a waterproof barrier when you shower.
Up to 40% of surgical procedures worldwide can be complicated by SSIs, making them the third-leading cause of healthcare-associated infections. These infections nearly double hospital stays and quadruple readmission risks, with almost half of all cases being preventable through evidence-based strategies. You can review more research about the global impact of SSIs and prevention on frontiersin.org.
Knowing the Early Warning Signs of Infection
Your body has its own alarm system for when things go wrong. Your job is to listen carefully and know what to look for. Most SSIs start to show symptoms within the first 3 to 7 days after surgery, but it's important to stay vigilant even after that window.
Keep a close eye on your incision site for any of these changes:
- Spreading Redness or Swelling: Some initial redness is normal, but it should get better over time, not spread out or get darker.
- Pain That Gets Worse: Post-op pain should gradually fade. If it suddenly intensifies or starts throbbing, that’s a major red flag.
- Warmth at the Incision: An infected area often feels noticeably warmer to the touch than the skin around it.
- Drainage or Pus: Any discharge that looks cloudy, yellow, or green is a clear sign of trouble. A foul smell is also a serious warning.
- Fever: A temperature of 100.4°F (38°C) or higher could mean your body is fighting off a larger infection.
If you spot even one of these signs, don't wait to see if it gets better on its own. Call your surgeon’s office immediately. Catching an infection early often means it can be handled with a simple course of antibiotics, preventing a minor issue from escalating into a serious complication. In some clinical settings, advanced tools like a point-of-care wound imaging device can even help clinicians spot elevated bacterial loads before a crisis develops.
Supporting Your Body's Healing Power
Beyond just caring for the wound itself, your overall health habits are a huge piece of the healing puzzle. Your body needs the right fuel and the right conditions to repair itself and fight off germs.
Think of your recovery as your body's full-time job. To help it perform at its best, stick to the plan laid out in your discharge instructions, especially in these areas:
- Nutrition: Your body is rebuilding tissue, which requires extra calories, protein, and vitamins. Focus on a balanced diet filled with lean proteins, fruits, and vegetables.
- Hydration: Water is absolutely essential for good circulation, which is how oxygen and nutrients get delivered to your wound. Drink plenty of fluids all day long.
- Rest and Activity: Listen to your body and follow every activity restriction. Pushing yourself too hard can strain the incision, but getting enough rest lets your body channel its energy directly into healing.
Following these guidelines isn't just about feeling comfortable; it’s an active strategy for preventing infection. By creating the best possible internal environment for healing, you give your body the upper hand in closing the wound quickly, leaving no opening for bacteria to move in.
Recognizing When to Seek Advanced Wound Care
While diligent post-operative care is your first line of defense, sometimes a surgical wound just doesn't follow the textbook healing process. Knowing when to call in a specialist is crucial. It’s about preventing a minor healing delay from spiraling into a major complication that threatens the patient's recovery.
If a surgical incision isn't showing clear signs of improvement after two weeks, it's time for a much closer look. A wound that hits a plateau—or worse, starts to regress—often needs more than standard care can offer. This is particularly true for patients with underlying health issues like diabetes or vascular disease, which can seriously hamper the body's ability to heal.
Red Flags That Signal a Need for a Specialist
Most surgical wounds heal just fine with standard protocols. But certain warning signs demand a specialist's intervention. Don't adopt a "wait and see" approach with these issues; quick action is the key to getting healing back on track.
Keep an eye out for these indicators:
- A Stalled Wound: If you see no reduction in size or visible improvement over a 14-day period, you're likely dealing with a chronic, non-healing wound.
- Spreading Signs of Infection: Redness that creeps far beyond the incision, persistent warmth to the touch, or red streaks moving away from the wound are all signs that an infection is advancing.
- Recurrent Drainage: Some clear or pinkish drainage is normal at first. But if you see persistent pus-like discharge, especially after a round of antibiotics, it points to a deeper, unresolved problem.
- Increasing Pain: Post-op pain should steadily decrease. If the pain at the wound site suddenly gets worse or becomes severe, that's a major red flag.
Ignoring these signs can lead to much more serious problems, including deep tissue damage or even systemic infection. A wound care specialist has the tools to find the root cause and deploy advanced diagnostics to figure out what’s really going on.
Advanced Diagnostics: Uncovering the Real Problem
One of the most common reasons a wound fails to heal is a stealthy, undiagnosed infection. Specialists have access to diagnostic tools that go way beyond what the naked eye can see, giving them a clear picture of the microbial battlefield in the wound bed.
A great example is fluorescence imaging. Using a device like the MolecuLight DX, we can shine a specific wavelength of light on the wound, making bacterial colonies glow in real-time. This isn't just a party trick; it allows us to see the exact location and bioburden of contamination, which makes for far more targeted and effective debridement.
Another game-changer is rapid pathogen testing. Forget waiting days for traditional cultures to come back from the lab. These modern tests can identify the specific bacteria causing an infection—and just as importantly, their antibiotic sensitivities—often within a few hours. You can read more about how clinics use advanced pathogen detection to accelerate their decision-making. That speed is invaluable for choosing the right antibiotic from day one and avoiding the trial-and-error approach that lets an infection dig in deeper.
Innovative Treatments for Complex Wounds
Once we have an accurate diagnosis, we can bring in advanced therapies designed to jump-start healing in even the most stubborn wounds. These treatments work with the body's own regenerative processes to create the ideal environment for tissue repair.
For instance, amniotic membrane allografts are proving to be a revolutionary tool for complex wounds. These grafts serve as a natural scaffold, delivering the essential growth factors and structural proteins needed to rebuild healthy tissue. A triple-layer allograft, in particular, provides a robust matrix that encourages new cell growth and can help close wounds that have failed every other treatment.
These advanced interventions are becoming central to modern wound care. From an economic standpoint, surgical site infections are the second most common healthcare-associated infection and are tied to a four-fold increase in hospital readmissions. Specialty wound care tackles this head-on. By using fluorescence imaging for precise cleaning, rapid pathogen ID for effective antibiotic selection, and triple-layer allografts to rebuild tissue, we can dramatically reduce healing times and the administrative burden on providers. For a deeper dive, check out the economic and clinical impact of advanced wound care on xiahepublishing.com. Knowing when to escalate care isn't just good medicine; it's essential for ensuring a safe and complete recovery.
Of course. Here is the rewritten section, crafted to sound like it was written by an experienced human expert, following all the provided guidelines.
Your Top Questions About Preventing Surgical Site Infections
Even with the best surgical plan, it's natural to have questions as you prepare for an operation or navigate your recovery. Let's walk through some of the most common concerns I hear from patients. My goal is to give you clear, straightforward answers so you can feel confident and in control of your care.
How Much of This Is Really Up to Me?
It’s a fair question. While the surgical team has total control over the sterile environment inside the operating room, your role as the patient is absolutely critical, especially before you even get to the hospital and after you go home. Your actions have a direct and powerful impact on your risk of infection.
Think of it as a true partnership. Before your surgery, your job is to:
- Be an open book. Tell your surgeon everything about your health history, medications, and habits like smoking. No detail is too small.
- Follow pre-op instructions to the letter. This means diligently using the antiseptic washes they give you, keeping your blood sugar in a tight range if you're diabetic, and stopping smoking as far in advance as possible.
- Protect your skin. Don't shave the surgical area yourself—this can create tiny nicks that harbor bacteria. Your job is to keep that skin intact and healthy.
Once you're home, you become the primary guardian of your wound. This is a huge responsibility. It means practicing meticulous hand hygiene every time you go near the incision, following wound care instructions precisely, and keeping a close eye out for any red flags.
Can I Just Use My Regular Soap or Lotion Before Surgery?
I strongly advise against it. It's best to stick exclusively to what your surgical team recommends in the days leading up to your procedure. Many everyday soaps, moisturizers, and even deodorants contain ingredients that can completely undermine the effectiveness of pre-surgical antiseptic cleansers like chlorhexidine gluconate (CHG).
These products often leave behind a residue. This film can either neutralize the antiseptic's germ-killing power or, worse, trap bacteria right against your skin. For the best possible outcome, use only the products your care team provides or specifically approves for the 24 hours before your surgery.
The Goal: We're trying to create the cleanest possible canvas for the surgeon to work on. Following the specific skin prep protocol is a simple but incredibly powerful way to lower the bacterial count on your skin and reduce your infection risk.
What Do I Do If I Think I Have an Infection?
If you spot any warning signs—we’re talking spreading redness, pain that’s getting worse instead of better, warmth around the incision, any kind of foul-smelling drainage, or a fever over 100.4°F (38°C)—do not wait. Call your surgeon's office immediately.
It’s a common mistake for patients to think, "I'll just give it another day and see if it gets better." This is a gamble you don't want to take. Early intervention is everything. An issue that could be resolved with a simple course of oral antibiotics can quickly escalate into a serious problem requiring hospitalization or another surgery if it's ignored. When it comes to post-op concerns, there is simply no such thing as being "too cautious."
The sheer scale of surgery performed each year really puts this into perspective. Globally, surgeons perform over 300 million procedures annually. Standardizing these simple prevention measures could prevent nearly half of all potential SSIs. We have solid data showing that when healthcare teams consistently follow evidence-based practices, infection rates drop significantly. You can read more about how prevention bundles reduce SSI rates on xiahepublishing.com.
Ultimately, your active participation is a non-negotiable part of a safe surgical outcome. By understanding your role and keeping an open line of communication with your healthcare team, you empower yourself to have the smoothest, healthiest recovery possible.
If you're dealing with a wound that just isn't healing right, don't wait for it to become a crisis. The team at Specialty Wound Care combines advanced diagnostics with expert clinical care to get you on the fastest path to recovery. Learn how our targeted treatments can make a difference at https://specialtywoundcare.com.